Download
1 / 64
640 likes | 726 Vues
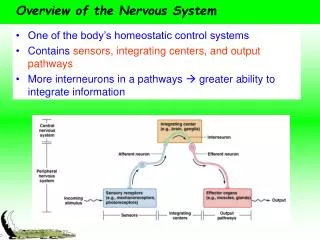
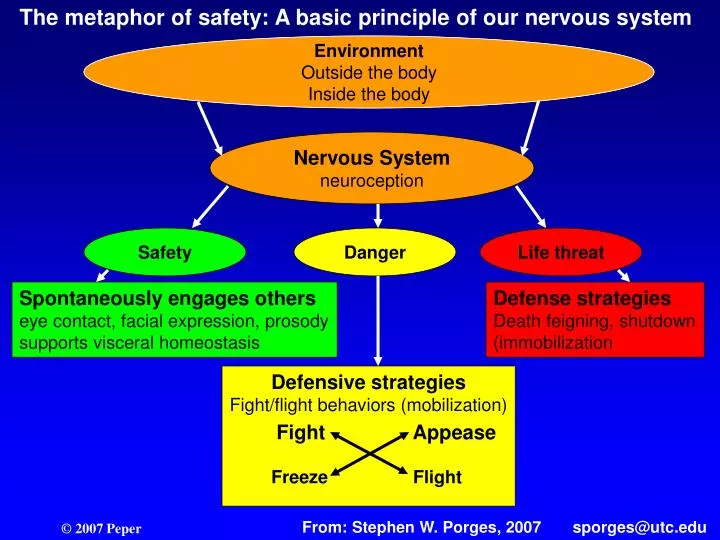
The metaphor of safety: A basic principle of our nervous system. Environment Outside the body Insidte the body. Environment Outside the body Inside the body. Nervous System neuroception. Safety. Danger. Life threat. Spontaneously engages others

E N D
The metaphor of safety: A basic principle of our nervous system Environment Outside the body Insidte the body Environment Outside the body Inside the body Nervous System neuroception Safety Danger Life threat Spontaneously engages others eye contact, facial expression, prosody supports visceral homeostasis Defense strategies Death feigning, shutdown (immobilization Defensive strategies Fight/flight behaviors (mobilization) Fight Appease Freeze Flight From: Stephen W. Porges, 2007 sporges@utc.edu
Under threat, evolutionary dissolution occurs the reverse of evolution--the phylogenetically determined hierarchy that regulates behavioral and physiological adaptation to safe, dangerous and life threatening environments. From: Stephen W. Porges, 2007 sporges@utc.edu
Stress • The “LOAD” on a system • A state of anxiety produced when events and responsibilities exceed one’s coping abilities (R. Lazarus) • The inability to cope with a perceived, real or imagined threat to one’s mental physical, emotional, and spiritual well-being which results in a series of physiological responses and adaptations (B. Seaward) • The non-specific response of the body to any demand placed upon it to adapt
Hans Selye’s Model: General Adaptation Syndrome • Alarm • Resistance • Exhaustion • Termination
Stage 1 - Alarm Stage • Physiological changes prepare body to fight, flee, or otherwise resist the stressor. • Physiological changes also known as the ‘fight or flight’ response.
Disruption of Homeostasis (the body's internal balance) processes • Regain its normal equilibrium once the stress has passed • Become stuck in an over aroused state. • Become stuck in an under aroused state • How a person copes with stress -- by reaching for a beer or cigarette as opposed to heading to the gym -- also plays a big role in the impact stress will have on our bodies. --Bruce McEwen and Dean Krahn
Stage 2 - Adaptation Stage • Changes of stage 1 appear to disappear but energy must be expended to resist the stressor. • Hormonal changes remain.
Allostasis and Allostatic Load • Allostasis are the adaptive responses which means maintaining stability, or homeostasis, through change. • Allostatic load is the price the body has to pay for either doing its job less efficiently or simply being overwhelmed by too many challenges. --Bruce McEwen and Dean Krahn
Stage 3 - Exhaustion Stage • Signs of alarm reaction return but there is no more energy to resist the stressor. Physiological systems begin to break down • Collapse or death if stressor is not removed.
Termination If there is no relief from the arousal, the resultant stress on the physiological systems lead to death of the organism.
Multi-dimension loading-capacity model Risk=______Load_______ Carrying ability Hagenaars, L.H.A., Bernards, A.T.M.& Oostendorp, R.A.B. (2002). The Multidimensional load/carriability Model. Amersfoort, Netherlands:Nederlands Paramedisch Instituut (Dutch National Institute of Allied Health Professions), , 2002, ISBN 90-73054-78-8
Human Performance Curve Nixon, P. & King, J. (1997). Ischemic heart disease: Homeostasis and the heart. In: Watkins, A. (ed.). Mind-Body Medicine. New York: Livingstone. Nixon, P.G.F. (1989). Human functions and the heart. In: Seedhouse, D. and Cribb, A. (eds). Changing Ideas in Health Care. New York: John Wiley & Sons
Hormonal pattern during arousal Catabolic hormones increase Anabolic hormones decrease Cortisol Insulin Epinephrine Calcitonin Glucagon Testoterone Antidiuretic hormone Prolactin Renin Luteinizing hormone Angiotensin Follicle stimulating hormone Aldosterone Gondatropin release hormone Erythropoietin (GnRH) Thyroxine Prolactin releasing hormone (PRH) Parathormone Estrogen Melatonin (Nixon, 1989)
Catabolic State (1 of 2) • Halt in synthesis of protein, fat, and carbohydrate • Increased breakdown of protein, free fatty acids, low density lipoprotein, cholesterol for energy) • Increased production of red blood cells and liver enzymes for energy • Decreased repair and replacement of bone (Nixon, 1989)
Catabolic State (2 of 2) • Decreased repair and replacement of cells with normally high turnover (gut, skin, etc.) • Decreased production of cells for immune system (thymus shrinks, circulating white cells decrease) • Decreased sexual processes • Increased blood pressure, cardiac output • Increased salt and water retention • Impaired digestion (Adapted from: Nixon, 1989)
AnabolicState • Increased synthesis of protein, fat, carbohydrate (growth, energy storage) • Decreased breakdown of protein, fat, carbohydrate (growth, energy storage) • Increased production of cells for immune system (white blood cells of thymus and bone marrow) • Increased bone repair and growth • Increase in sexual processes (cellular, hormonal, and psychological) • Improved digestion (Adapted from: Nixon, 1989)
Am I on the Downslope?* (1 of 2) • Because too much is demanded of me? • Because I cannot say ’no’ when necessary? • Because I am not sufficiently in control? Can’t cope? • Too angry, too tense, too upset, too irritable, too indignant? • Too much people-poisoning?(caring for too many people and then having nothing left for family members) • Too many time-pressures? • Too impatient? *Nixon, P. & King, J. (1997). Ischemic heart disease: Homeostasis and the heart. In: Watkins, A. (ed.). Mind-Body Medicine. New York: Livingstone.
Am I on the Downslope?* (2 of 2) • Because I am not sleeping WELL enough to keep well? • Because I am not keeping fit enough to stay well? • Because I am not balancing the periods of hard effort with adequate sleep and relaxation? • Because I am out of real energy and using sheer willpower to keep going? • Because I am infallible, indispensable, indestructible, and/or immortal? *Nixon, P. & King, J. (1997). Ischemic heart disease: Homeostasis and the heart. In: Watkins, A. (ed.). Mind-Body Medicine. New York: Livingstone.
The Protesting Body* • What is it trying to say? Am I listening? • Why is it protesting? • What makes it protest each time? And why so often? • Am I working to make it stronger or am I too upset with myself to succeed? • Am I looking for a drug/operation to keep it quiet? *Nixon, P. & King, J. (1997). Ischemic heart disease: Homeostasis and the heart. In: Watkins, A. (ed.). Mind-Body Medicine. New York: Livingstone.
Travell, J.G. and Simons, D. G. (1983). Myofacial Pain and Dysfunction The Trigger Point Manual. Baltimore: Williams & Wilkins
Changes, Purposes, and Long-term Consequences of During Stress
Two Components of Illness • Actual pathophysiology • Panic/worry/fear/helplessness One can always reduce panic/worry/fear and thereby encourage the self-healing
True Emergency False Emergency Perception of Danger Misperception of danger Reduce stimuli Change perception Skill mastery Somatic/cognitive awareness Actions to increase control, safety, and social support Physical movement Relaxation Regeneration Return to homeostatic balance Fight/flight/freeze response Energy Mobilized Action No action Emergency resolved Energy discharged Energy bound Regeneration Neuromuscular tension and autonomic arousal Return to homeostatic Resistance balance Exhaustion Termination
Fight/flight versus Freeze • Possible gender differences? • Women tend and befriend (nurture and seek support) • Man tend towards aggression or escape • Possible explanation of higher incidence of whiplash and chronic illness in women? • Women more shortness of breath: fear/freeze • Man more heart attacks: anger and hostility
Women 'tend and befriend' while men 'fight or flee‘* Females of many species, including humans, respond to stressful conditions by protecting and nurturing their young, and by seeking social contact and support from others -- especially other females. Stressed-out women are likely to seek social contact, rather than indulge in the "fight-or-flight" behavior that has long been considered the principal way both sexes cope with stress. Possible impact: Males reduce social capital. Females increase social capital. Social capital is positively correlated with health. Is this why males die sooner? *Shelley Taylor, UCLA, 2000
From: Melton, L. (2002). His pain, her pain. New Scientist. 2326, 32-35
From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Four Mood States on Two Arousal Continuums • Calm-energy • Calm-tiredness • Tense-energy • Tense-tiredness From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Calm-energy (Good mood) • Cardiovascular system in slight arousal, respiration and heart rate slightly elevated, metabolic rate increased • Time of day mid-day and after having eaten breakfast with protein and no simple carbohydrates • Feeling in a good mood, peppy and vigorous, confident, sociable, ability to focus on work and no urgency, just a quiet and relaxed attention From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Calm-tiredness • Cardiovascular system at low level of arousal, respiration and heart rate slightly reduced, metabolic rate decreased • Time: Late evening relaxing, not much active thinking • Feeling in a good mood although less intense than in calm-energy, quiet, sleepy or drowsy From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Tense-energy • Cardiovascular system in slight arousal, respiration and heart rate slightly elevated, metabolic rate increased, increase in muscle tension in the jaw, shoulders, neck and back, freeze reaction • Danger or a threat of danger is near • A sense of pressure, time pressure and urgency (e.g., deadlines). Thoughts are more distracting and scattered • Feelings of energy, pep and vigor with tension and jitteriness (low level of anxiety); fast efficient work From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Tense-tiredness (Bad mood) • Exhaustion, poor sleep the night before, more coffee and sweets and no exercise, fatigue mixed with nervousness • Time: Possibly late in the afternoon. Tendency to eat snacks and drink coffee. Negative thoughts and the future looks bad. At night, tossing and turning while trying to go to sleep • Feelings of exhaustion and negative thoughts keep arising. Insignificant hassles have major impact More likely to occur when energy is low 4 pm and 9-11 pm From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Index of tense-tired (1-2) • What is the time of day? • How much sleep have I got recently? • When did I eat last (and what kind of food did I consume)? • Have I been sedentary for a long period (when did I exercise last)? • How good is my general health? • What is my general stress level? From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Index of tense-tired (2-2) • (For women) What time of month is it? • Have I recently been taking psychoactive drugs (including alcohol), or am I avoiding psychoactive drugs (including nicotine and caffeine) on which I have become dependent? • What is my current energy level? • What is my current tension level? From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Exercise increases energy • Moderate exercise immediately increases energy (observe that as begin to walk and walk a bit more rapidly ones energy will begin to rise) • Secondarily, exercise will reduce some tension and general elevation of optimism From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Food effects energy • Hunger reduces energy • Sugar initially increases energy and after one hour energy level dropped and tension level increased (energy level rated lower than before eating sugar—a sense of fatigue sets in). From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Engel, G. L., Ferris., E.G. & Logan, M. (1947). Hyperventilation: Analysis of clinical symptomatology. Annals of Internal Medicine. 27 (5), 690.
From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Self-control of mood: Ranking of efficacy • Active mood management: Relaxation, stress management, engage in cognitive activity, exercise • Seeking pleasure activity and distractions: Engage in pleasant activities such as humor or a hobby • Withdrawal-avoidance: Be alone, avoid person or thing causing bad mood • Social support, ventilation and gratification: Call or talk to someone, engage in emotional activity, smoke, eat • Passive mood management: Watch TV, drink coffee, eat, rest • Direct tension reduction: Take drugs, drink alcohol, have sex From: Thayer, R.E. (1996). The Origin of Everyday Moods. New York: Oxford University Press.
Assessment Protocol • General stress assessment • Specific task/job/illness related assessment • Make assessment meaningful • Analyses suggests solutions • Implementing solutions enhances health • Issues of time—how long an assessment
Purpose of Assessment • Identify risk factors that participant can use to enhance health • Demonstrate to the participant that risk is present and behavior change can reduce risk • Do intervention • Collect pre/post data
What to remember • Most assessments are idiosyncratic and developed by clinicians / researchers / educators. • I most cases there is no evidence that this assessment is any better than another assessment. • Most are useful for practitioner / clients • Questions how the collected data impacts training and impacts outcome
Two examples of Assessment • Assessment at the computer • Assessment of poker dealers
Procedure • Place hands on lap and relax (30 seconds). • Lift hands allowing fingers to rest on the middle (home) row of keys (30 seconds). • Begin data entry by typing a standardized text (1 minute). • Stop typing and rest fingers on the home row (30 seconds). • Place hands on lap and relax (30 seconds). • Rest hand on mouse (30 seconds). • Begin mousing by repeatedly cutting the last word of the text and pasting it to the beginning of the text as quickly as possible (60 seconds). • Stop mousing and rest hand on mouse (30 seconds). • Place hands on lap and relax (30 seconds). • Remember a negative emotionally event (e.g., a time when you were angry). • When the memory/event is felt, nod your head and begin the second typing task while holding the emotional memory (60 seconds). • Stop typing, place your hand on your lap and relax, letting go of the emotional experience (30 seconds).
Published Protocol • Peper, E., Harvey, R. & Tylova, H. (2006). Stress protocol for assessing computer related disorders. Biofeedback. 34 (2), 57-62. http://www.aapb.org/files/public/57-62_BIOF3402-Peper.pdf • Peper, E. & Gibney, K. H. (2006). Muscle Biofeedback at the Computer: A Manual to Prevent Repetitive Strain Injury (RSI) by Taking the Guesswork out of Assessment, Monitoring and Training. Amersfoort: The Netherlands: Biofeedback Foundation of Europe. ISBN 0-9781927-0-2