Download
1 / 52
550 likes | 626 Vues
Innate Immunity: Inflammation. Chapter 6. Immunity. First line of defense

E N D
Innate Immunity: Inflammation Chapter 6
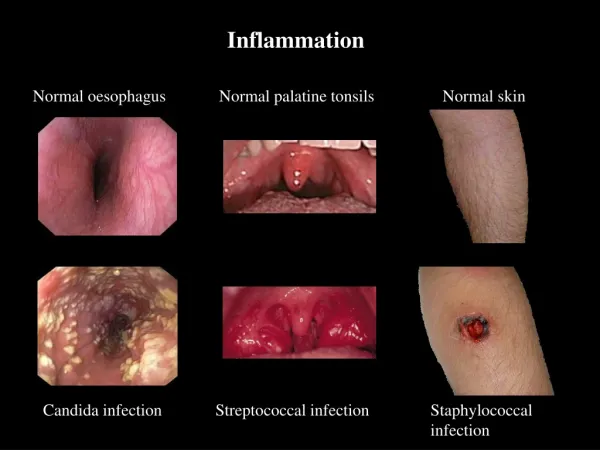
Immunity • First line of defense • Innate resistance – physical (skin/epithelial layer, GI & Resp Tract), , mechanical (Cough, sneeze, vomit, cilia action in trachea) & biochemical barriers (antimicrobial peptides, lung secretions, mucus, saliva, tears, earwax) • Second line of defense • Inflammation – vascular response – dilation, histamines increase vessel leakage, wbc action, cytokines, leucokines, fever. Usually redness and heat with swelling. • Third line of defense • Adaptive (acquired) immunity – antibody production
First Line of Defense • Physical and mechanical barriers • Skin • Linings of the gastrointestinal, genitourinary, and respiratory tracts • Sloughing off of cells • Coughing and sneezing • Flushing • Vomiting • Mucus and cilia
First Line of Defense • Biochemical barriers • Synthesized and secreted saliva, tears, earwax, sweat, and sebum • Antimicrobial peptides • Cathelicidins, defensins, and collectins • Normal bacterial flora
Second Line of Defense • Inflammatory response • Caused by a variety of materials • Infection, mechanical damage, ischemia, nutrient deprivation, temperature extremes, radiation, etc. • Local manifestations • Vascular response • Blood vessel dilation, increased vascular permeability and leakage, white blood cell adherence to the inner walls of the vessels and migration through the vessels
Inflammation • Goals • Limit and control the inflammatory process • Prevent and limit infection and further damage • Interact with components of the adaptive immune system • Prepare the area of injury for healing
Plasma Protein Systems • Protein systems • Complement system • Coagulation system • Kinin system • All contain inactive enzymes (proenzymes) • Sequentially activated • First proenzyme is converted to an active enzyme • Substrate of the activated enzyme becomes the next component in the series
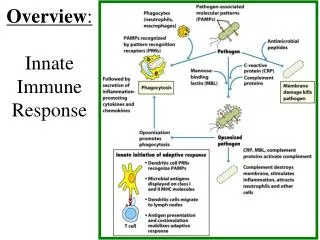
Plasma Protein Systems • Complement system • Can destroy pathogens directly • Activates or collaborates with every other component of the inflammatory response • Pathways • Classical • Lectin • Alternative
Plasma Protein Systems • Coagulation (clotting) system • Forms a fibrinous meshwork at an injured or inflamed site • Prevents the spread of infection • Keeps microorganisms and foreign bodies at the site of greatest inflammatory cell activity • Forms a clot that stops bleeding • Provides a framework for repair and healing • Main substance is an insoluble protein called fibrin
Plasma Protein Systems • Kinin system • Functions to activate and assist inflammatory cells • Primary kinin is bradykinin • Causes dilation of blood vessels, pain, smooth muscle contraction, vascular permeability, and leukocyte chemotaxis
Cellular Mediators of Inflammation • Cellular components • Granulocytes, platelets, monocytes, and lymphocytes • Cell surface receptors • Pattern recognition receptors (PRRs) • Pathogen-associated molecular patterns (PAMPs) • Toll-like receptors • Complement receptors • Scavenger receptors
Mast Cells • Cellular bags of granules located in the loose connective tissues close to blood vessels • Skin, digestive lining, and respiratory tract • Activation • Physical injury, chemical agents, immunologic processes, and toll-like receptors • Chemical release in two ways • Degranulation and synthesis of lipid-derived chemical mediators
Mast Cell Degranulation • Histamine • Vasoactive amine that causes temporary, rapid constriction of the large blood vessels and the dilation of the postcapillary venules • Retraction of endothelial cells lining the capillaries • Receptors • H1 receptor (proinflammatory) • H2 receptor (anti-inflammatory)
Histamine • Receptors • H1 receptor • Proinflammatory • Present in smooth muscle cells of the bronchi • H2 receptor • Anti-inflammatory • Present on parietal cells of the stomach mucosa • Induces the secretion of gastric acid
Mast Cell Degranulation • Chemotactic factors • Neutrophil chemotactic factor • Attracts neutrophils • Eosinophil chemotactic factor of anaphylaxis (ECF-A) • Attracts eosinophils
Mast Cell Synthesis of Mediators • Leukotrienes • Product of arachidonic acid from mast cell membranes • Similar effects to histamine in later stages • Prostaglandins • Similar effects to leukotrienes; they also induce pain • Platelet-activating factor • Similar effect to leukotrienes and platelet activation
Phagocytosis • Process by which a cell ingests and disposes of foreign material • Production of adhesion molecules • Margination (pavementing) • Adherence of leukocytes to endothelial cells • Diapedesis • Emigration of cells through the endothelial junctions
Phagocytosis • Steps • Opsonization, recognition, and adherence • Engulfment • Phagosome formation • Fusion with lysosomal granules • Destruction of the target
Phagocytes • Neutrophils • Also referred to as polymorphonuclear neutrophils (PMNs) • Predominate in early inflammatory responses • Ingest bacteria, dead cells, and cellular debris • Cells are short lived and become a component of the purulent exudate
Phagocytes • Monocytes and macrophages • Monocytes are produced in the bone marrow, enter the circulation, and migrate to the inflammatory site, where they develop into macrophages • Macrophages typically arrive at the inflammatory site 3 to 7 days after neutrophils • Macrophage activation results in increased size, plasma membrane area, glucose metabolism, number of lysosomes, and secretory products
Phagocytes • Eosinophils • Mildly phagocytic • Duties • Defense against parasites and regulation of vascular mediators
Phagocytes • Natural killer (NK) cells • Function is to recognize and eliminate cells infected with viruses and some function in eliminating cancer cells • Platelets • Activation results in degranulation and interaction with components of the coagulation system
Cytokines • Interleukins • Produced primarily by macrophages and lymphocytes in response to a pathogen or stimulation by other products of inflammation • Many types • Examples • IL-1 is a proinflammatory cytokine • IL-10 is an anti-inflammatory cytokine
Cytokines • Interferon • Protects against viral infections • Produced and released by virally infected host cells in response to viral double-stranded RNA • Types • IFN-alpha and IFN-beta • Induce production of antiviral proteins • IFN-gamma • Increases microbiocidal activity of macrophages
Cytokines • Tumor necrosis factor–alpha • Secreted by macrophages in response to PAMP and toll-like receptor recognition • Induces fever by acting as an endogenous pyrogen • Increases synthesis of inflammatory serum proteins • Causes muscle wasting (cachexia) and intravascular thrombosis
Local Manifestations of Inflammation • Results from vascular changes and corresponding leakage of circulating components into the tissue • Heat • Redness • Swelling • Pain
Exudative Fluids • Serous exudate • Watery exudate: indicates early inflammation • Fibrinous exudate • Thick, clotted exudate: indicates more advanced inflammation • Purulent exudate • Pus: indicates a bacterial infection • Hemorrhagic exudate • Exudate contains blood: indicates bleeding
Systemic Manifestations of Inflammation • Fever • Caused by exogenous and endogenous pyrogens • Act directly on the hypothalamus • Leukocytosis • Increased numbers of circulating leukocytes • Increased plasma protein synthesis • Acute-phase reactants • C-reactive protein, fibrinogen, haptoglobin, amyloid, ceruloplasmin, etc.
Chronic Inflammation • Inflammation lasting 2 weeks or longer • Often related to an unsuccessful acute inflammatory response • Other causes of chronic inflammation: • High lipid and wax content of a microorganism • Ability to survive inside the macrophage • Toxins • Chemicals, particulate matter, or physical irritants
Chronic Inflammation • Characteristics • Dense infiltration of lymphocytes and macrophages • Granuloma formation • Epithelioid cell formation • Giant cell formation
Resolution and Repair • Regeneration • Resolution • Returning injured tissue to the original structure and function • Repair • Replacement of destroyed tissue with scar tissue • Scar tissue • Composed primarily of collagen to restore the tensile strength of the tissue
Resolution and Repair • Débridement • Cleaning up the dissolved clots, microorganisms, erythrocytes, and dead tissue cells • Healing • Filling in the wound • Sealing the wound (epithelialization) • Shrinking the wound (contraction)
Healing • Primary intention • Wounds that heal under conditions of minimal tissue loss • Secondary intention • Wounds that require a great deal more tissue replacement • Open wound
Healing • Reconstructive phase • Fibroblast proliferation • Collagen synthesis • Epithelialization • Contraction • Myofibroblasts • Cellular differentiation
Healing • Maturation phase • Continuation of cellular differentiation • Scar tissue formation • Scar remodeling
Dysfunctional Wound Healing • Dysfunction during inflammatory response • Hemorrhage • Fibrous adhesion • Infection • Excess scar formation • Wound sepsis • Hypovolemia • Hypoproteinemia • Anti-inflammatory steroids
Dysfunctional Wound Healing • Dysfunctional during reconstructive phase • Impaired collagen matrix assembly • Keloid scar • Hypertrophic scar • Impaired epithelialization • Anti-inflammatory steroids, hypoxemia, and nutritional deficiencies • Impaired contraction • Contracture
Dysfunctional Wound Healing • Wound disruption • Dehiscence • Wound pulls apart at the suture line • Excessive strain and obesity are causes • Increases risk of wound sepsis