Download
1 / 21
210 likes | 436 Vues
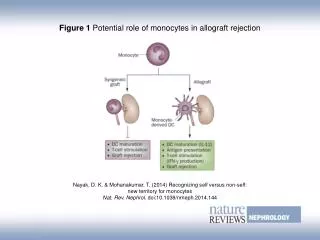
Complement in acute liver allograft rejection Eighth Banff Conference on Allograft Pathology Edmonton 2005 A. Dankof Institute of Pathology Universitätsmedizin Berlin, Charité. Introduction.

E N D
Complement in acute liver allograft rejection Eighth Banff Conference on Allograft Pathology Edmonton 2005 A. Dankof Institute of Pathology Universitätsmedizin Berlin, Charité
Introduction In the past the liver has been regarded to be resistant to antibody-associated rejection. Rejection mechanisms were accepted to be almost always based on T-cell mediated immunoresponse. (Michaelis et al., Springer Semin Immunopathol 2003) Several studies demonstrated an association of circulating anti-donor antibodies with rejection and graft loss. (Bishara et al., Hum Immunol 2002; Scornik et al., Am J Transplant 2001; Takakura et al., Clin Transplant 2001) B-lymphocytes in liver tissue obtained from one patient with ACR expressed a restricted Vh-gene repertoire with a selected pattern of somatic mutations. (Moeller et al., Virchows Arch 2005)
MAC and CD59 Conti F, Grude P, Calmus Y, Scoazec JY, Journal of Hepatology 1997
MAC and CD59 Lautenschlager I, Höckerstedt K, Meri S, Journal of Hepatology 1999
MAC and CD59 Lautenschlager I, Höckerstedt K, Meri S, Journal of Hepatology 1999
C4d N = 15 Pre LTX Immunohistochemical single staining C4d, CD20, CD138 LTX ACR N = 15 Krukemeyer M, Moeller J, Morawietz L, Rudolph B, Neumann U, Theruvath T, Neuhaus P, Krenn V, Transplantation 2004
C4d C4d C4d deposits were detected in severely inflamed portal tracts of 5 biopsies from patients with ACR (n=5).
CD20 CD20 CD138 CD138 B-lymphocytes and plasma cells Pre LTX ACR Pre LTX ACR
B-lymphocytes and plasma cells p(CD20) = 0.002 p(CD138) = 0.02
Immunohistochemical single staining C4d, CD68, CD20, CD38 Immunohistochemical/immunofluorescence double staining C4d/CD68 N = 13 Control N = 22 N = 22 ACR C4d Dankof A, Schmeding M, Morawietz L, Günther R, Krukemeyer M, Rudolph B, Koch M, Krenn V, Neumann U, Virchows Archiv 2005
C4d C4d p= 0.013 C4d
CD68/Macrophages * ** ACR/C4d+ CD68 *p = 0.007 **p = 0.007
C4d and CD68 CD68/C4d CD68/C4d
B-lymphocytes and plasma cells CD20 CD38 p(CD20) = 0.029 p(CD38) = 0.014
Control ACR HCV N = 29 N = 34 N = 34 Immunohistochemical single staining C4d C4d
C4d p<0,001
C4d mild moderate severe ACR ACR ACR N = 16 N = 14 N = 5 Immunofluorescence C4d Sawada T, Shimizu A, Kubota K, Fuchinoue S, Teraoka S, Clin Transplant 2005
C4d • Mild rejection detection of C4d in the portal areas in some cases • Moderate rejection detection of C4d in sinusoids, portal veins and portal arteries • Severe rejection detection of C4d in lobules and portal areas
Summary • C4d deposits are detectable in a great portion of patients with acute liver allograft rejection. • Detection of C4d is associated with an increased number of macrophages in the portal tracts. • The distribution pattern of C4d deposits and its association with rejection severity grade remain controversial.
Conclusion Immunologically there is more to acute liver allograft rejection than pure T-cell mediated immunoresponse. The detection of C4d supports the existence of humorally mediated mechanisms in acute liver allograft rejection.
Acknowledgements Department of Surgery, Charité Universitätsmedizin Berlin Ulf Neumann Maximilian Schmeding Peter Neuhaus Institute of Pathology, Charité Universitätsmedizin Berlin Gabriele Fernahl Raphaela Günther Janine Karle Martin Koch Manfred Krukemeyer Lars Morawietz Birgit Rudolph Veit Krenn