Download
1 / 35
450 likes | 912 Vues
Cell Mediated Immunity. W. Robert Fleischmann, Ph.D. Department of Urologic Surgery University of Minnesota Medical School rfleisch@umn.edu (612) 626-5034. Objectives. To understand the role of cell-mediated immunity

E N D
Cell Mediated Immunity W. Robert Fleischmann, Ph.D. Department of Urologic Surgery University of Minnesota Medical School rfleisch@umn.edu (612) 626-5034
Objectives • To understand the role of cell-mediated immunity • To understand the identity, mechanism of activation, and method of killing by cytotoxic T cells • To understand the identity, mechanism of activation, and method of killing by natural killer (NK) cells • To understand the method of killing by antibody-mediated cellular cytotoxicity (ADCC)
Arvak Petrosian, age 2 years, is brought from Armenia to a private clinic in the U.S. that specializes in diagnosis and treatment of unusual diseases. Arvak has a history of failure to gain weight. He appears to be anorexic. In addition, he is noted to have eczema. He has recently been diagnosed with Type I diabetes. According to his Armenian physicians, he is now showing signs of hypothyroidism. What are your thoughts? What tests would you wish to request?
A complete blood cell count shows Low levels of neutrophils Low levels of RBCs Low levels of platelets T and B cell mitogen stimulation is normal. Antibody isotypes and sub-types are at normal levels. What are your thoughts? What tests would you wish to request?
Urinalysis shows the presence of protein in the urine. Blood chemistry shows elevated levels of serum creatinine and urea nitrogen. Liver enzymes are significantly elevated. What are your thoughts? What tests would you wish to request?
Arvak is diagnosed as having Eczema Enteropathy (destruction of cells in the intestine) Diabetes Neutropenia Anemia Thrombocytopenia Thyroiditis Glomerulonephritis Hepatitis What are your thoughts?
Role of Cell-Mediated Immunity • Humoral immunity mediated by antibody is responsible for the protection of the extra-cellular environment from pathogens and toxins. • The principal roles of cell-mediated immunity are to recognize and destroy pathogen-infected cells and cells that have undergone genetic alterations (tumor cells). • The importance of cell-mediated immunity can be seen in patients who lack a thymus (DiGeorge Syndrome). • Although antibodies are not made, these patients deal relatively well with extracellular bacteria. • DiGeorge patients do suffer repeated infections because no memory. • Infections with viruses, intracellular bacteria, and fungi are difficult to clear and become life-threatening in DiGeorge patients.
The Mediators of Cell-Mediated Immunity • Antigen-nonspecific effector cell • Natural Killer cells • Macrophages • Neutrophils • Eosinophils • Antigen-specific effector cells • CD4+ T cells (aka, helper T cells, Th cells) • CD8+ T cells (aka, cytotoxic T cells, CTLs, Tc cells)
Different Effector T Cells Can Be Recognized by the Effector Molecules They Produce
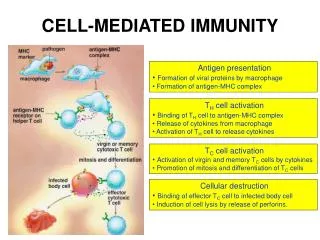
Cytotoxic T Cells • Naïve CTL cells are called CTL precursors (CTL-P) to indicate their immature state. • A CTL-P cell matures only after being activated by interaction with a Th1 cell. • Maturation requires three sequential signals. • Antigen-specific signal is transmitted by the TCR upon recognition of peptide:Class I antigen presented by a professional antigen presenting cell (licensed antigen-presenting cell) or by a tissue cell. • Costimulatory signal is transmitted by CD28:B7 interaction between the CTL-P cell and the licensed antigen-presenting cell. • A signal induced by IL-2 secreted by a Th1 cell, results in proliferation and differentiation of the antigen-activated CTL-P cell to a CTL.
Activation of Effector CTLs from Naïve CTL-Ps • Before an APC can activate a CTL-P cell by peptide:MHC class I presentation, it must be “licensed” to do so. • APC must present peptide via MHC Class II to a Th1 cell. • Somehow, this interaction licenses the APC to present peptide via MHC Class I antigen to the CTL-P cell. • It is not known whether the Th1 cell and the CTL-P cell are bound to the APC at the same time. Note: Naïve CTL-P = naïve CTL precursor
Importance of Licensing of APC • Licensing of APC requires interaction of the APC with the Th1 cell. • Thus, presentation of antigen to the Th1 cell via MHC class II and to the CTL-P cell via MHC class I acts a control to prevent recognition of self antigen (antigen must be a phagocytosed antigen to be expressed on Class II). • This is a function best carried out by a dendritic cell acting as an APC. • Infection of a dendritic cell by a virus assists in the presentation of antigen associated with MHC class I.
Activation of Memory CTLs • Th1 cell not required to provide IL-2. • Autocrine IL-2 is sufficient.
Naïve CTL-P Does not express IL-2 or IL-2R and only begins to express them after it begins to be activated. Expresses the CD45RA isoform of CD45. Expresses a low level of cell adhesion molecules CD2 and LFA-1. Does not exhibit cytotoxic activity. Mature CTL Expresses high affinity IL-2 receptor and requires high levels of IL-2 to proliferate. Synthesizes low levels of IL-2. Expresses the CD45RO isoform of CD45. Expresses a high level of cell adhesion molecules CD2 and LFA-1 Exhibits cytotoxicity. Memory CTL cells may not require Th1 help. Requires only low levels of IL-2 (produced by activated CTL-Ps) for memory CTLs to become mature effector CTLs. Naïve CTL-P Versus Mature CTL
Overview of CTL Killing • Primary events • Conjugate formation • Reorientation of cytoplasmic granules in CTL • Granule exocytosis • Dissociation • Target cell death by apoptosis
Pictures of CTL Killing Note that the T cell approaches the target cell, forms a close binding to the target cell, and reorients its granules (small arrow) toward the target cell.
CTL Killing: Binding of Target Cell • The TCR-CD3 membrane complex on the CTL recognizes peptide bound to MHC class I on a target cell. • LFA-1 on CTL binds to ICAMs on target cell. • Antigen activation converts LFA-1 from a low-affinity state to a high-affinity state, resulting in the formation of the conjugate. • After 5-10 minutes, the LFA-1 returns to a low-affinity state, resulting in dissociation of the CTL from the target cell.
Bound CTLs Kill Targets by Two* Mechanisms • Perforin/Granzyme are secreted from granules • Perforin molecules form pore • Granzyme molecules activate apoptosis by cleavage of caspases • FasLigand protein on cell membrane surface • Membrane-bound FasL binds to Fas on the membrane of the target cell to initiate cell killing • Activates apoptosis by cleavage of caspases * CTLs can also kill by TNF production and secretion
CTL Killing: Degranulation Events • The CTLs (but not naïve CTL-Ps) contain intracellular granules. • Contain monomers of perforin • Perforin monomers polymerize to form pore in the target cell • Perforin has some homology with C9 and forms pores similar to complement pores • Contain serine proteases called granzymes or fragmentins • Granzymes taken up by receptor mediated endocytosis (granzyme binds to mannose 6-phosphate receptor) or through perforin pore (perforin-assisted pathway) • Granzymes induce apoptosis
Apoptosis Inductionby FasL and Granzyme • FasL on the CTL binds to Fas (TNF family receptor) on the target cell, activating its death domains to bind to FADD (FAS-associated Death Domain) that, in turn, activates caspase-8 • Granzymes initiate apoptosis by activating caspase-8
Natural Killer Cells (NK Cells) • NK cells make up 5-10% of the population of circulating lymphocytes. • NK cells play major roles in killing virus-infected cells, intracellular pathogen-infected cells, and tumor cells. • NK cells produce a number of important cytokines, including IFN-. • IFN- can tilt the immune response toward Th1 cells by inhibiting Th2 and by inducing IL-12 production by macrophages and dendritic cells. • IFN- can activate macrophages and NK cells. • NK cell activity is stimulated by IFN-, IFN-, IFN-, TNF-, IL-12 and IL-15.
NK Cells versus CTLs • NK cells express CD16, FcRIII. • NK cells do not need to be educated by the thymus. • NK cells do not undergo rearrangement of receptor genes and, thus, do not express T cell receptors or CD3. • NK cell killing is not MHC restricted (identical killing levels are seen for allogeneic and syngenic tumor cells). • NK cells do not show immunologic memory that can be primed by re-exposure to antigen. • NK cell killing is similar to CTL killing • FasL expressed on surface and can kill cells expressing Fas • Perforin and granzyme released from granules • TNF expressed on surface and secreted
NK Cell Receptors • NK cells have both activation and inhibition receptors. • NK cell receptors fall into two categories but members of each group can be activation or inhibition receptors. • Lectin-like receptors • Bind proteins rather than polysaccharides • Can be activation or inhibition receptors • Immunoglobulin-like receptors (aka, KIR = killer cell immunoglobulin-like receptors) • Bind to most class I MHC molecules • Can be activation or inhibition receptors, but most are inhibition receptors
Opposing Signals Model ofNK Cell Killing • If an antigen recognition signal is given to the NK cell and the level of MHC class I is high, no killing occurs. • If an antigen recognition signal is given to the NK cell and the level of MHC class I is low, killing occurs.
NK Cells Kill cells that mask the presence of foreign antigen on MHC class I CTLs Kill cells that express foreign antigen on MHC class I NK Cells and CTL Have Complementary Activities
NKT Cells • NK cells express lectin-like receptors and KIR. • CTL express T cell receptor and CD3. • NKT cells express T cell receptor but differs from CTL. • Maturation is in the thymus. • The T cell receptor is invariant (specific gene segments encode TCR and TCR chains). • The T cell receptor does not recognize MHC-bound peptides but does recognize a glycolipid presented by CD1d. • NKT cells do not exhibit memory. • NKT cells express cell surface markers characteristic of NK cells. • NKT cells may play a role in killing bacteria and tumor cells but precise role is uncertain. • Bacteria killing via expression of glycosyl ceramides (glycolipid)? • Tumor cell killing via expression of glycolipids that are specific to tumor cells?
ADCC Killing • Effector cells associated with ADCC • NK cells • Macrophages • Monocytes • Neutrophils • Eosinophils • Effector cells bind antigen via antibody bound to Fc receptor • Killing is mediated by • Cytolytic enzyme release by macrophages,neutrophils,and eosinophils • TNF release by NK cells, monocytes, and macrophages • Perforin release by NK cells and eosinophils • Granzyme release by NK cells
Arvak Petrosian Because of the number of organ systems under autoimmune attack, Arvak is diagnosed with a rare condition called IPEX syndrome (immune dysregulation, polyendocrinophathy, enteropathy, X-linked syndrome). This syndrome is caused by mutations in the FOXP3 gene.
Arvak Petrosian FOXP3 gene function is required for the development of Treg cells. In the absence of appropriate Treg cell function, CD8+ cytotoxic T cells are active and destroy normal tissue cells that they recognize. Thus, peripheral tolerance is lost, resulting in autoimmunity.