Download
1 / 8
90 likes | 406 Vues
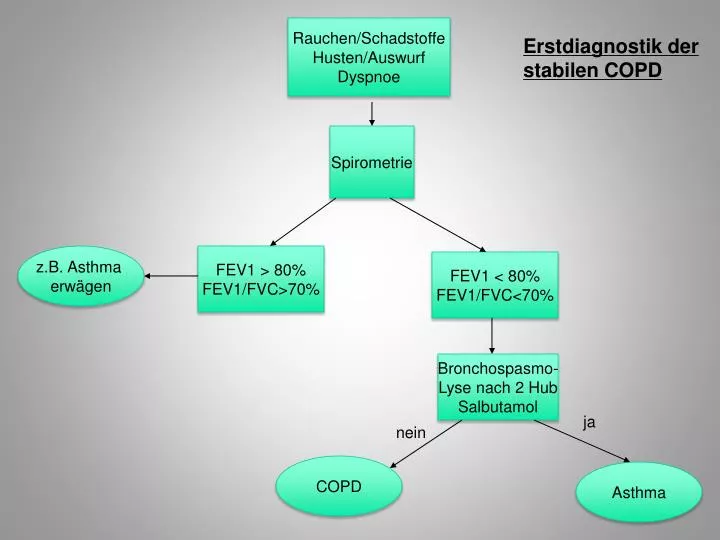
Rauchen/Schadstoffe Husten/Auswurf Dyspnoe. Erstdiagnostik der stabilen COPD. Spirometrie. z.B. Asthma erwägen. FEV1 > 80% FEV1/FVC>70%. FEV1 < 80% FEV1/FVC<70%. Bronchospasmo- Lyse nach 2 Hub Salbutamol. ja. nein. COPD. Asthma. COPD. COPD-Stadieneinteilung

E N D
Rauchen/Schadstoffe Husten/Auswurf Dyspnoe Erstdiagnostik der stabilen COPD Spirometrie z.B. Asthma erwägen FEV1 > 80% FEV1/FVC>70% FEV1 < 80% FEV1/FVC<70% Bronchospasmo- Lyse nach 2 Hub Salbutamol ja nein COPD Asthma
COPD COPD-Stadieneinteilung und Primärtherapie Stadiierung I II III IV Stadiengerechte Einleitung der Therapie DMP/Schulung Tabakentwöhnung Überweisung Facharzt
COPD - Differenzialdiagnostik COPD Röntgen-Thorax Bodyplethysmographie Blutgasanalyse Definitive Stadieneinteilung Leitliniengerechte Therapieempfehlung
Leitliniengerechte Stadieneinteilung und Therapie der COPD Schweregrad I leicht II mittel III schwer IV sehr schwer Charakteristika • FEV1 / VC <70% • FEV1 ≥ 80% • mit / ohneSymptomatik • FEV1 / VC <70% • 50%≤FEV1<80% • mit / ohneSymptomatik • FEV1 / VC <70% • 30%<FEV1<50% • mit / ohne Symptomatik • FEV1 / VC <70% • FEV1≤30% • FEV1 <50% und chron. respiratorische Insuffizienz, Zeichen der Rechtsherz-insuffizienz Vermeidung von Risikofaktoren, Grippe- und Pneumokokken-Schutzimpfung, zusätzlich bei Bedarf kurzwirksamen Bronchodilatator Zusätzlich Dauertherapie mit einem oder mehreren langwirks. Bronchodilatatoren, Rehabilitation Zusätzlich inhalative Glukokortikoide bei wiederholten Exazerbationen Zusätzlich Langzeit- O2-Therapie bei resp. Insuffizienz. Prüfen ob chirurg. Behand-lung angezeigt ist Mod. nach Leitlinie der Deutschen Atemwegsliga COPD 2007
COPD - Kontrollen COPD DMP: alle 6 Monate Spirometrie Stadien I + II Stadien III + IV Alle 6 Monate Spirometrie Alle 12 Monate Body Alle 3 Monate Body, ggf BGA
Unzureichender Therapie- effekt COPD- unzureichender Therapieeffekt Differenzial- Diagnosen erwägen besser/ Lungenfunktions- kontrolle schlechter/ Exazerbation? siehe dort unauffällig idem schlecht Inhalationstechnik ? Adäquates Device? schlecht Compliance ? Neuschulung Therapie- anpassung Bodykontrolle ggf.BGA ggf Röntgen
Auskultation Spirometrie ggfs. Oximetrie COPD –Exazerbation Zunahme von Dyspnoe, Sputummenge und Sputumpurulenz pathologisch ? RÖ 2 Ebenen ja nein Andere Ursachen erwägen Keine Pneumonie Pneumonie s. dort GOLD I&II Therapie- Eskalation je nach Vormedikation Tiotropium LABA Theophyllin ß-Lactame Tetrazyklin Antibiose über 5-7 Tage GOLD III&IV ß-Lactam + Inhibitor Cephalosporin II/III Gyrasehemmer IV Prednisonäquivalent 40 mg/die 3-tägige Dosishalbierung
COPD - Therapieversagen beiExazerbation Zeichen der Pneumonie ? Pneumonie Keine Pneumonie CRB 65 Index ? *** ambulant stationär • *** CRB 65 Index:- Bewusstseinstrübung • Atemfrequenz>30/min- diast. RR < 60/ syst.RR < 90 mmHg- Alter >65Jahreab 1 Punkt Einweisung erwägen! stationär Röntgen, BGA, Body