Download
1 / 52

E N D
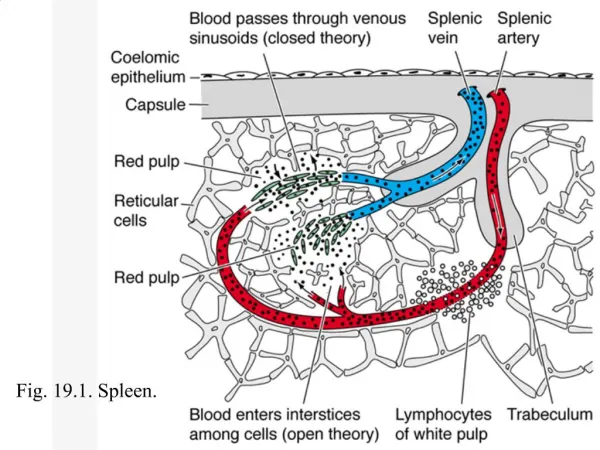
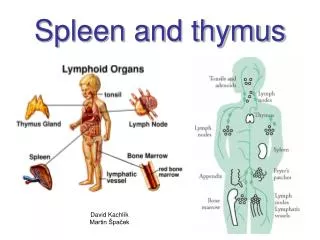
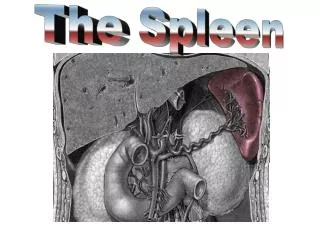
1. The Spleen
2. Anatomy of Spleen
3. White Pulp
5. Spleen Structure
The white pulp is circular in
structure and is made up mainly
of lymphocytes. It functions in a
manner similar to the nodules of the
lymph node.
The red pulp surrounds the white
pulp and contains mainly red blood
cells and macrophages. The main
function of the red pulp is to
phagocytize old red blood cells.
6. Red Pulp
7. Function The spleen is a sophisticated filter that monitors and manages blood cells and immune functions
During fetal development the spleen produces red and white blood cells
By the fifth month of gestation the spleen no longer has hematopoietic function but retains the capacity throughout life
Red cells that pass through the spleen undergo a �cleaning� or repair
Abnormal and old cells are destroyed
8. Function Reticulocytes loose their nuclear remnants and excess membrane before entering the circulation
RBC�s coated with IgG and IgM are removed and destroyed
The spleen is the site of destruction in autoimmune disease states (ITTP and hemolytic anemia)
Parasites such as malaria can be removed as well
The spleen is involved in specific and nonspecific immune responses (promotes phagocytosis and destruction of bacteria)
9. Sites of Haemopoiesis Yolk sac
Liver and spleen
Bone marrow
Gradual replacement of active (red) marrow by tissue inactive (fatty)
Expansion can occur during increased need for cell production
Embryonic haemopoietic stem cells-mesenchymal cells in yolk sac
After 12 week fetal liver and spleen becomes the main site
From week 20, bone marrow starts to become important and by the time of birth it is the main haemopoietic organEmbryonic haemopoietic stem cells-mesenchymal cells in yolk sac
After 12 week fetal liver and spleen becomes the main site
From week 20, bone marrow starts to become important and by the time of birth it is the main haemopoietic organ
11. Splenic Trauma Diagnosis
Injury should be suspected in blunt upper abdominal injuries ( MVA and Bike)
Injuries are often associated with fractured ribs of the left chest
Splenic injuries can cause extensive and continued hemorrhage, others can cause subcapsular hematomas that are subject to rupture at any time
If splenic injury is suspected, admission to the hospital for monitoring is mandatory
The signs and symptoms of splenic trauma are those of hemoperitoneum (generalized LUQ pain)
12. Treatment of Ruptured Spleen Splenic preservation operations
Partial splenectomy
Capsular repair
Non operative treatment
13. Delayed Rupture of the Spleen Injury to the pulp sometimes cannot be contained indefinitely by the splenic capsule
The usual interval between injury and hemorrhage is within two weeks (longer intervals have been reported)
The incidence is between 15-30%
It is hoped that as imaging techniques improve the incidence will decrease
14. Splenosis Is the auto transplantation of splenic tissue after splenic trauma
They vary from a few millimeters to several centimeters in diameter
May occur anywhere in the peritoneal cavity
Seldom causes symptoms and is usually discovered as an incidental finding at reoperation
Post splenectomy sepsis has renewed interest in splenosis
15. Causes of splenomegaly Infection
Bacterial: Typhoid fever, endocarditis, septicemia, abscess
Viral:E-B virus, CMV, and others
Protozoal: Malaria, toxoplasmosis
Hematologic processes
Hemolytic anemia: Congenital, acquired
Extramedullary hematopoiesis: thalassemia, osteopetrosis, myelofibrosis
Neoplasms
Malignant: Leukemia, lymphoma, histiocytoses, metastatic tumors
Benign: Hemagioma, hamartoma
Metabolic diseases
Lipidosis: Niemann-Pick, Gaucher disease
Mucopolysaccharidosis infiltration: Histiocytosis
Congestion
Cirrhosis
Cysts
Miscellaneous
16. Hypersplenism Refers to a variety of ill effects resulting from increased splenic function that may be improved by splenectomy
The criteria for diagnosis included:
Anemia, leukopenia, thrombocytopenia or a combination of the three
Compensatory bone marrow hyperplasia
Splenomegaly
Hypersplenism can be categorized as primary or secondary
17. Splenic Involvement in Hodgkin�s lymphoma The probability of splenic involvement increases with increasing spleen size
The absence of splenomegaly does not exclude splenic involvement
Upon gross examination of the spleen a grayish white nodule ranging from several millimeters to several centimeters is apparent with Hodgkin�s disease
Liver involvement with Hodgkin�s disease rarely occurs in the absence of splenic disease
18. Felty�s Syndrome Is a syndrome consisting of severe rheumatoid arthritis, granulocytopenia and splenomegaly
It usually occurs in patients with a long history of rheumatoid arthritis
Severe, persistent and recurrent infections are characteristic
Moderate splenomegaly is common
Splenectomy is effective in most patients
19. Gaucher�s Disease Is a disorder of lipid metabolism that may result in massive splenomegaly and hypersplenism
Commonly found in the Jewish population
Diagnosis is made by finding the typical Gaucher�s cells in biopsy tissue
Massive splenomegaly is usually the most common form of presentation
The adult form is the most common form
Splenomegaly (subtotal) shows great benefits
21. Cysts and Tumors of the Spleen The differential diagnosis of splenomegaly should include splenic masses and primary tumors (these conditions are rare however they must be considered)
Cystic lesions comprise parasitic and nonparasitic cysts
Parasitic cysts are due almost exclusively to echinococcal disease (rare in the United States)
Nonparasitic cysts are classified as primary (true) which have an epithelial lining or pseudocysts (more common
Symptoms of splenic cysts are vague and are caused primarily by mass effect (compression of adjacent viscera)
22. Cysts and Tumors of the Spleen Selected nonparasitic cyst may be managed by aspiration
Splenectomy should be performed for all large cyst and those with an uncertain diagnosis
Malignant and benign primary tumors of the spleen are rare
Most primary malignant tumors are angiosarcomas
23. Infectious Mononucleosis A disease characterized by fever, sore throat, lymphadenopathy and atypical lymphocytes
Most patients are young
Clinical symptoms are similar to those of a severe upper respiratory tract infection
The spleen is enlarged and palpable in over 50% of patients
Splenic rupture may occur
24. Incidental Splenectomy The spleen is vulnerable to injury during operative procedures in the upper abdomen
When the splenic capsule is torn, splenectomy is frequently performed
Morbidity and mortality is higher with iatrogenic injury requiring splenectomy
25. Splenectomy Prior to removing the spleen specific preoperative preparation is necessary
All patients should receive polyvalent pneumococcal vaccine, polyvalent meningococcal vaccine and Haemophilus influenzae type b conjugant vaccine
Blood and blood products should be available well in advance of surgery
26. Blood Compositional Changes in the Asplenic or Hyposplenic Patient The absence of functional splenic tissue results in characteristic changes in the circulating blood
Some of these are predictable and desirable results
These changes are considered a measure of its success when splenectomy is performed for a hematologic disease
Howell-Jolly bodies (nuclear remnants) and thrombocytosis (desired result)
Other findings include: target cells, acanthocytes (spur cells), Heinz bodies (denatured hemoglobin) and stippled red cells
27. Postsplenectomy Sepsis Asplenic patients have an increased susceptibility to the development of overwhelming infection
The risk of sepsis is approximately 60 times greater than normal after splenectomy
The risk is greatest in children younger than four years of age
The risk of sepsis is higher among patients requiring splenectomy for inherited diseases
The risk of sepsis after splenectomy is lowest after trauma
28. Postsplenectomy Sepsis Postsplenectomy sepsis syndrome typically occurs in a previously healthy individual after a mild upper respiratory tract infection associated with fever
Within hours, nausea, vomiting, headache, confusion, shock and coma can occur; death follows within 24 hours
The nature of the syndrome makes it difficult to diagnose early enough for therapy to be effective
29. Postsplenectomy Sepsis The most common bacteria isolated our streptococcus pneumoniae, Neisseria meningitidis, E. coli or Haemophilus influenzae
Because half of the patients develop sepsis from strep pneumoniae, penicillin can be administered immediately with onset of a febrile URI
Patients are instructed to obtain and wear a Medic alert tag
30. Hyposplenism Is a potentially lethal syndrome characterized by diminished splenic function
The patient peripheral blood smears appear as if they are asplenic
Hyposplenism can occur in the presence of abnormal sized or enlarged spleen
The danger of hyposplenism is the risk of developing potentially lethal sepsis
Sickle cell anemia is the most common disease associated with hyposplenism
The most common surgical disease associated with hyposplenism is chronic UC
31. Hyposplenism
32. Overview Definition of Hyposplenism
Medical History
The function of the spleen
Congenital asplenia vs. splenectomy
Immunological consequences of Hyposplenism
Diagnosis and complications
33. What is Hyposplenism? Hyposplenism is the lack of a spleen or its function
The rare genetic disorder- Congenital Asplenia
The surgical removal of the spleen- splenectomy
Results in severe immunological consequences.
34. History Immunological importance of the spleen
Morris and Bullock-1919
First post-splenectomy infection
O�Donnell-1929
Effects of Hyposplenism
King and Shumacker-1952
35. The Spleen Largest lymphoid tissue of the body
Serves two main functions
Filters blood to remove damaged/old RBC- red pulp
Serves as secondary lymphoid tissue by removing infectious agents and using them to activate lymphocytes- white pulp
A significant reservoir for T lymphocytes
Plays an active role in the production of IgM antibodies and complement
Has significant role in the functional maturation of antibodies
36. Congenital Asplenia Autosomal recessive genetic disorder
Believed to be caused by absence of the Hox 11 gene in the embryo
Causes decreased adaptive immune response
Associated with structural abnormalities in other organs of the body- cause death in infancy
37. Splenectomy Removal of spleen tissue (partial or complete)
Usually needed because of trauma
Residual splenic function in � to ? of patients
IgM levels decreases, IgG levels remain constant or increase, IgA and IgE levels increase
38. Immunological Consequences Causes slower and incomplete adaptive immune response against bacteria
Low levels of tuftsin, which stimulates phagocytosis by neutrophils, macrophages, and monocytes
Decreased neutrophil and macrophage activity
Increased NK cell activity
Limited capacity of circulating B-cells to differentiate into antibody-secreting cells
Decreased level of T-cells
39. Diagnosis Determined by anatomic presence or absence of the organ, its size, and any lesions.
Function can be assessed by
Radiologic Techniques
X-ray, ultrasound, tomography, MRI, radionucleotide scanning
Morphologically
Peripheral blood smear- presence of Howell-Jolly bodies
40. Howell Jolly bodies Howell-Jolly
bodies are round, purple staining nuclear fragments of DNA in the red blood cell
41. Complications Lifelong risk for Overwhelming Postsplenectomy infection (OPSI)
Caused by Streptococcus pneumoniae and gram negative bacteria
Initial Symptoms: fever, chills, muscle aches, headache, vomiting, diarrhea, and abdominal pain
Progressive symptoms: bacteremic septic shock, extremity gangrene, convulsions, and coma
Mortality rate of 50-80%
from onset of initial symptoms, 68% of those deaths occur within 24 hours and 80% occur within 48 hours
Prevention: routine vaccinations and prophylactic antibiotics
42. Summary Hyposplenism is the lack of a spleen or its function
Can be either genetic or surgically induced
It has detrimental effects on the immune system by decreasing the body�s ability to fight bacterial infections and reducing the adaptive immune response
43. Infections in Asplenic Patients
44. Causes of Asplenia Congenital
Often associated with serious organ malformations
Acquired
Post surgical removal
Functional hyposplenism
45. Function of the Spleen Immunological functions
Main site of opsonic antibody production
Especially efficient in removal of encapsulated bacteria
Remaining RES may compensate but not in case of encapsulated bacteria
Filtration
Removal of abnormal erythrocytes and intraerythrocytic inclusions eg nuclear inclusions and parasitised RBC
46. Overwhelming Infection Overall incidence of sepsis is low
3,2% in adults
3,3% in children
Risk stratified according to cause, being highest in patients with thalassaemia major and sickle-cell anaemia (J Infect 2001 Oct;43: 182-6)
Lifetime risk for OPSI of 5%
Mortality
Death rates 600 times greater than general population
Higher in children (1,7% vs 1,3%), but other reports say higher in > 16 years
Mandel say doesn�t correspond to indication but Bisharat et al suggest higher in haematological disorders
47. Duration of risk Most occur within 2 years post splenectomy
Risk is lifelong as cases have been reported up to 20 years post surgery
Early complications may be underreported as surgical complication
48. Microbiology S. pneumonia
50 � 90% of cases
Common in all age groups
Distribution of serotypes seems to be same as other forms of pneumococcal infection
75% belonged to serotypes covered in 23 valent vaccine (ibid)
49. Micro cont� H. influenza
Regarded as 2nd most common cause
Incidence reduced with vaccination
Non-typable strains do not seem to predominate in PSS
N. meningitidis
Reported by some studies as associated but others as well as animal experiments seem to support a lack of association
50. Other Micro-organisms Listeria monocytogenes
E. coli
Klebsiella sp
Salmonella typhimurium
S. aureus
Cytocapnophagia canimorsus
Plesiomonas shigelloides
Recently occupational exposures have been highlighted
51. Management Immunisations
Pneumococcal � 2 weeks prior to elective surgery otherwise when patient is recovered prior to discharge. Boosters every 5-10 years
H. influenza � recommended but evidence for immunogenicity and boosters lacking
Meningococcal � not routinely recommended
Influenza � may be of value especially in reducing risk of secondary bacterial infection
52. Mx continued� Antibiotic prophylaxis
Controversial
Penicillin
In all cases, esp in first 2 years post surgery
All up to 16 and if underlying immune dysfunction
May not prevent sepsis
Local resistence patterns need to accounted for
Home antibiotic supply
53. Cont��� Travellers
MALARIA PROPHYLAXIS
Meningococcal vaccine
Antibiotic prophylaxis
Education
Medic alert bracelet etc.