Download
1 / 45
470 likes | 940 Vues
ELECTRONIC FETAL HEART RATE MONITORING: Where are we and where are we going?. Gary D. V. Hankins, M.D. The University of Texas Medical Branch Special thanks – Dr. George Macones and Dr. Cathy Spong. ELECTRONIC FETAL HEART RATE MONITORING: A Reevaluation Workshop April 28-29-2008

E N D
ELECTRONIC FETAL HEART RATE MONITORING: Where are we and where are we going? Gary D. V. Hankins, M.D. The University of Texas Medical Branch Special thanks – Dr. George Macones and Dr. Cathy Spong
ELECTRONIC FETAL HEART RATE MONITORING: A Reevaluation Workshop April 28-29-2008 Co-sponsored by the Pregnancy and Perinatology Branch (PPB) at the National Institute of Child Health and Human Development, The American College of Obstetricians and Gynecologists (ACOG) And The Society for Maternal Fetal Medicine (SMFM)
Represented • NICHD – PPB • SMFM • ACOG • ACNM • AWHONN • AAP • RCOG • CCOG • National Cardiovascular Center - Japan
Breakout Groups • Group 1: Systems (two vs three vs five tiers) Rationale implications • Group 2: Definitions of FHR patterns Baseline FHR Baseline FHR variability Acceleration • Group 3: Definitions of FHR patterns Late deceleration Early deceleration Variable deceleration Prolonged deceleration
‘The RCOG System – 2001’ • ‘The use and interpretation of cardiotocography in intrapartum fetal surveillance’ • RCOG Evidence-based Clinical Guideline No 8 • Adopted by National Institute of Clinical Excellence (NICE) • Published for May 2001 • For this Workshop focus on terminology used in EFM Courtesy of Dr. David James
Four arguments for development ofEFM Guideline • Intrapartum hypoxia • 1% of all labors • 10% perinatal deaths - CESDI (Confidential Enquiry into Stillbirths and Deaths in Infancy) • IP hypoxic death rate = 0.8:1000 births • 10% CP cases • IP hypoxic CP rate = 0.1:1000 births Courtesy of Dr. David James
Four arguments for development ofEFM Guideline • EFM use • 239/248 (96.4%) maternity units in UK use EFM • 26% did not have an EFM Guideline (30% in units > 3000 dels) • Fetal blood sampling used in 88% Courtesy of Dr. David James
Four arguments for development ofEFM Guideline • Suboptimal EFM use • CESDI (Confidential Enquiry into Stillbirths and Deaths in Infancy) 70% of IP deaths have Grade II/III suboptimal care • Majority of examples relate to EFM • Failure to recognize • Failure to act • Communicate failure Courtesy of Dr. David James
Four arguments for development ofEFM Guideline • Medicolegal issues • > $800 million estimate of NHS medicolegal costs currently • > 60% are obstetric cases • Majority of obstetric cases relate to fetal monitoring in labor Courtesy of Dr. David James
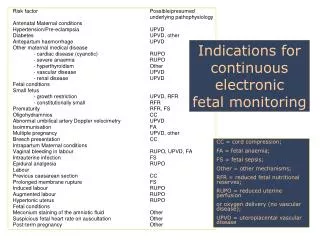
Risk categories for fetal acidemia related to FHR variability, baseline rate and presence of recurrent decelerations. VD, Variable decelerations; LD, Late decelerations; PD, Prolonged decelerations; Brd, Bradycardia; Tachy, Tachycardia G, Green; B, Blue; Y, Yellow; O, Orange
EFM Interpretation Systems • 1997 NICHD: 2 tier • RCOG: 3 tier • Extensive vetting and peer review • National implementation, 50% drop in intrapartum death rate • SOGC: 3 tier • Extensive vetting and peer review • Miller: 3 tier • Least stringent • Common sense approach • Definition, interpretation, management • Parer: 5 tier • Applied knowledge, interdisciplinary • Variability driven
Outline of Workshop Findings Assumptions Describing FHR tracing components Categories of the new 3 tier system Meaning and actions required for each tier
Assumptions (1) • The definitions were developed for visual interpretation of FHR patterns. Computerized interpretation is not yet mainstream. • Both FHR and uterine activity should be of adequate quality for visual interpretation.
Assumptions (2) • Episodic patterns are those not associated with uterine contractions. • Periodic patterns are those associated with uterine contractions • Characterized as either “abrupt” or “gradual” onset • No distinction is made between short term and long term variability
Assumptions (3) • FHR tracings should be evaluated in context of clinical conditions including: • gestational age, • medications, • maternal medical conditions, and • fetal conditions (eg, growth restriction, known congenital anomalies, fetal anemia, arrhythmia etc).
Assumptions (4): An EFM tracing requires qualitative and quantitative description of: Uterine contractions Baseline FH rate Baseline FHR variability Presence of accelerations Periodic or episodic decelerations Changes or trends of FHR patterns over time
Describing Contractions • Number of UCs per 10 minute window • Averaged over 30’ • Normal: ≤ 5 contractions in 10’ • Tachysystole: > 5 contractions in 10’ • Presence or absence of decelerations • Spontaneous and stimulated labor • Hyperstimulation and hypercontractility are to be abandoned.
Describing FHR Baseline Rounded to 5 bpm Assembled from segments of baseline totaling at least 2’ in the 10’ window Excludes periods of accelerations, decelerations and hypervariability Bradycardia is < 110 bpm Tachycardia is > 160 bpm
Describing FHR Variability Excludes accelerations, decelerations Quantitated as peak-to-trough Absent variability: amplitude undetectable Minimal variability: amplitude detectable but ≤ 5 bpm Moderate variability: amplitude 6-25 bpm Marked variability: amplitude > 25 bpm
Describing Accelerations • Abrupt increase in FHR • Onset to peak < 30” • Peak: ≥ 15 bpm lasting 15” from onset to return to baseline • Prolonged acceleration: ≥ 2’ but < 10’ • Acceleration > 10’ = baseline change
Describing Decelerations • Decreasein FHR associated with uterine contraction • Gradual decrease: onset to nadir ≥ 30” • Abrupt decrease: onset to nadir < 30” • Recurrent decelerations: • Occurs with ≥ 50% of UCs • Intermittent decelerations: • Occurs with < 50% of UCs
Deceleration Features NOT Defined Slow return to baseline Biphasic decelerations ‘Reflex’ tachycardia following variable decelerations Shoulders or overshoots FHR fluctuations in the trough of the deceleration Mild, moderate and severe
What to Call the Categories? • Problems • Limited evidence base • Litigation issues • Possible titles: • Normal, reassuring, non-pathological • Abnormal, pathological • Intermediate, suspicious, non-reassuring, atypical • Conference Decision: • Reassuring • Equivocal – requires ongoing assessment/evaluation; • Abnormal – requires urgent action
After Extensive Discussion: • Concerns about terms: normal, abnormal, equivocal • Concerns about implied action necessary (e.g., equivocal requires intervention). • Final Framework: • Category I • Category II • Category III
3 Tier FHR Interpretation System:Category I Category I FHR tracings include allof the following: Baseline rate:110-160 bpm Baseline FHR variability: moderate Late or variable decelerations: absent. Early decelerations: present or absent. Accelerations: present or absent.
3 Tier FHR Interpretation System:Category III • Category III FHR tracings include either: • Absent FHR variability andany of the following: • Recurrent late decelerations • Recurrent variable decelerations • Bradycardia • Sinusoidal Pattern for ≥ 20’
3 Tier FHR Interpretation System:Category II Category II FHR tracings includes all FHR tracings not categorized as Category I or Category III. Represent an appreciable fraction of those encountered in clinical care.
3 Tier FHR Interpretation System:Category II Examples Moderate variability with bradycardia Minimal FHR variability Absent variability with no recurrent decels Recurrent variable decels with moderate variability Recurrent late decels with moderate variability
FHR Management Principles Correlate with fetal acid-base status Do NOT predict cerebral palsy Are only relevant for the point in time referenced
FHR Categories: Meaning and Action • Category I • Normal • Strongly predictive of normal acid base status • Follow ‘in a routine manner’ • Category III • Abnormal • Predictive of abnormal acid base • Prompt evaluation required • Resolve the pattern (support measures, delivery)
FHR Categories: Meaning and Action • Category II • Indeterminate • Not predictive of abnormal acid base status • Inadequate evidence to classify as Category I or III • Requires evaluation, continued surveillance and reevaluation