Download
1 / 45
600 likes | 1.74k Vues
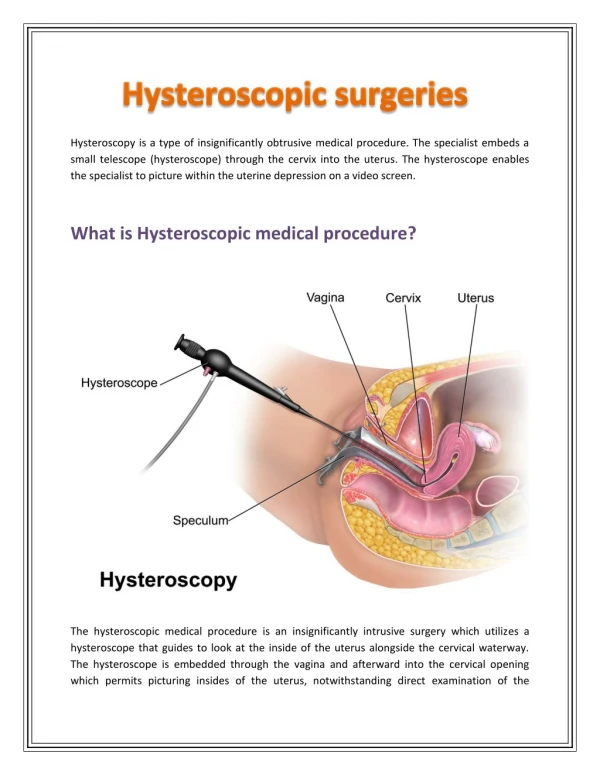
Complications of Hysteroscopy. Franklin D. Loffer , M.D. Executive Vice President/Medical Director A A G L “Advancing Minimally Invasive Gynecology Worldwide”. Uterine Perforation. Diagnostic (1° in office) 1/4000 0.03% Ablation/resection 69/5748 1.2% Submucous myoma 7/968 0.7%

E N D
Complications of Hysteroscopy Franklin D. Loffer, M.D. Executive Vice President/Medical DirectorA A G L “Advancing Minimally Invasive Gynecology Worldwide”
Uterine Perforation Diagnostic (1° in office) 1/4000 0.03% Ablation/resection 69/5748 1.2% Submucous myoma 7/968 0.7% Adhesions 1.0% Septum 1.0% AAGL survey 1988/1991/1993 1.3 / 1.1 / 1.4% F D Loffer literature review
Prevention of Uterine Perforations • Good visualization • Adequate distension • Not resecting below uterine cavity • Ultrasound or laparoscopy monitoring
Problems from PerforationDuring Hysteroscopy • Partial - increased fluid intravesation - lost orientation • Complete - procedure discontinued - bleeding (vaginal and/or abdominal) - intrabdominal organ injury higher with thermal energy sources than mechanical.
Hemorrhages Submucousmyomas 2.2% Endometrial ablation/resection 0.5%*- 0.8% AAGL survey 1988/1991/1993 0.1/0.03/0.25% FD Loffer literature review
Causes of Hemorrhage • Deep myometrial vessels • Uterine or cervical artery and branches • Intraabdominal vessels • Not from: - superficial myometrial vessels - transection of submucous fibroids - fundal perforation
Managing P.O. Hemorrhage • Tincture of time (wait and see) • Dilute pitressin (3 mgm / 10 cc) • Balloon / Foley • Pitressin pack
Types of Distention Media • Gas: CO2 • High viscosity fluid • Dextran 70 • Low viscosity fluid • Glycine • Sorbitol • Mannitol • Saline / Ringers Lactate
Problems From Fluid Overload • Congestive heart failure (all media) • Hyperammonemia (glycine) • Coagulopathies and/or allergic reactions (dextran) • Hyponatremia/hypo-osmolarity → death (electrolyte free media)
Fluid Intravasation Is : • The loss of uterine distending media into open uterine vessels • Most critical with electrolyte free media • Less critical with electrolyte media
Frequency of Fluid Overload • AAGL survey - 1988 0.34% - 1991 0.14% - 1993 0.2% • Submucous myoma 1.1% • Endometrial ablation / resection 1.5% FD Loffer Literature Review
Direction of Flow Relates to Pressure more less equal Pressure in: Uterus BloodVessel less A more B equal C (in fluid at rest the pressure is equal everywhere in the system)
Amount of Flow Relates to Pressure(with equal hole size) Pressure = 2x Pressure = 4x
Amount of Flow Relates to Hole Size(with equal pressure) Pressure = 4x Pressure = 4x
Relation Between Fluid Loss, Operative Time & Myomas Emanual, et al., “An analysis of fluid loss during transcervical resection of submucous myomas”, Fertility & Sterility. 68:5, 1997 pp. 881-886
Relative Pressures(approximate) • Uterine distension - 50 – 70 mm Hg • Fallopian tubes open - 55 – 110 mm Hg • Mean arterial blood pressure - 120/70 mm Hg
Fluid Management • Fluid management is required for operative hysteroscope • Manual calculation is inadequate - Approximately 10% error in fluid packaging - Time delays - Nursing calculation errors
Fluid Delivery /Monitoring Systems • Gravity vs. mechanical pumps(pressure is pressure) • Eyeball vs. measuring(seeing is not believing)
Fluid Delivery /Monitoring Systems • Pumps – Convenience • Monitoring – Early warning – Exact amounts – Evaluating rapidity Value of:
Osmolality of Distending Media • Glycine 1.5% 200 mOsmol/l • Sorbitol 3% - Mannitol 0.5% 178 mOsmol/l • Mannitol 5% 280 mOsmol/l (Normal serum osmolality 290 mOsmol/l)
Cerebral Edema Following Absorption of Glycine Irrigating Solution [H2O] Intravascular half-life 85 minutes [H2O] [H2O] [H2O] Vascular space Interstitial space Intracellular space A B Skull Brain Brain [H2O] Skull [H2O] [H2O] [H2O] H2O crossesblood-brain barrier C D Interstitial space Intracellular space
Is Mannitol A BetterMedia Than Glycine? 1½% Glycine 5% Mannitol pt 1 pt 2 pt 1 pt 2 Vol. Deficit (L) 2.124 2.448 3.640 2.735 P.O. Na (mmol/L) 124 124 105 110 Na diff (mmol/L) 18 15 36 31 Serum osmolality diff (mmol/L) -13 -11 1 -3 Nausea & vomiting + + 0 0 Phillips, DR et al. JAAGL 1997;4:567
5% Mannitol Metabolism • Metabolism • Absorption 6-10% • Excretion 90-94% • Plasma half life 15-102 min • Excessive intravasation • Hypervolemia • Hyponatremia • Normal plasma osmolality
Intravasation Increased By • Open vascular channels • High infusion pressure • High flow rate • Long operative time
Trendelenberg positioning is not necessary and should be avoided in hysteroscopy
Diagnosing Gas Embolism • end tidal CO2 • Millwheel murmur • central venous pressure • cardiac output • Doppler echocardiography
Hysteroscopic Venous Gas Embolization- Critical Issues • Room air • Products of combustion • Volume
Carbon Dioxide Embolism FollowingDiagnostic Hysteroscopy • 33 y/o - diagnosis: ectopic vs. SAB • L/S H/S @ 150 mm Hg + 100 ml/min • 4 min H/S D&C • Cardiac arrest from gas embolism4 min after H/S Brink, DM. Brit J OBG. 1994;101:717.
Compostion1 of Gases Found byHysteroscopic Electrosurgical Vaporization Bipolar Unipolar Air(normal saline) (glycine) Hydrogen 51.0 49.0 0.00005 CO 25.7 26.1 0.00001 CO2 6.5 7.5 0.0314 O2 2.9 3.0 20.9476 N 1.4 2.3 78.084 C2H2 3.6 4.1 CH4 2.8 2.5 0.0002 Misc2 6.0 5.6 -- -- 1 - Measured in mole percent 2 - Acetylene, Propane, C3 Olefin, Isobutane, n-Butane, C4 Alkene, C5 Hydrocarbon Munro et al. JAAGL Nov 2001
Toxicology and Solubility of Gases Formed By Electrosurgical Vaporization Solubility Toxic in Blood Risk to Pt Hydrogen low moderate volume only CO highhigh depends on amount CO2 low high little N low low volume only O2 none high volume only Munro et al. JAAGL Nov 2001
Frequency of Gas Embolization -Monopolar Resectoscope Using Glycine • Detected in hepatic vein or right heart - 3 control patients 0 - 11 operative patients 10/11 • No significant patient problems • Hepatic vein traps gas first Bloomstone et al. JAAGL Feb 2001
Avoiding Risks of Gaseous Intravesation • Purge air from lines • No Trendelenberg • Alert anesthesiologist • Protect open cervix • Avoid high pressures (intravasation) • Inadequate uterine flushing
Preventing Fluid Overload • Anticipate possibility of problem • Minimal distension pressures • Operate quickly • Use mannitol solution? • Use of oxytocin, vasopression or GnRh agonists? • Accurate intake & output
Conclusions • Fudalperferations carry a low risk unless accompanied by thermal injury. • Fluid intravesation is a major risk of hysteroscopy. • It occurs primarily in operative cases. • 5% Mannitol may be a better media.
ThankYou For Your Attention