Download
1 / 36
370 likes | 543 Vues
Do stretch activated ion channels have a physiological role in the heart?. Douglas Kelly Cellular Biophysics Laboratory Department of Physiology University of Adelaide. Investigation of MEF and the Frank-Starling relationship in the heart. Mechano-electric Feedback.

E N D
Do stretch activated ion channels have a physiological role in the heart? Douglas Kelly Cellular Biophysics Laboratory Department of Physiology University of Adelaide
Investigation of MEF and the Frank-Starling relationship in the heart
Mechano-electric Feedback • The electrical activity of the heart drives its mechanical activity • Excitation Contraction Coupling • Calcium-induced calcium release (CICR) • Changes in electrical activity can be brought about by changes in mechanical activity • Stretch activated ion channels MEF
Mechano-electric Feedback • Observations of cardiac rhythm disturbances and sudden death caused by non-penetrating mechanical impacts to the chest. • Post mortem sectioning shows no signs of internal or structural damage. • This condition is referred to as Commotio cordis ( disturbance of the heart).
Experimental work on Commotio cordis • Wooden hammers of varying weights and diameters used to apply impacts to the precordial region of anaesthetised animals. (Georg Schlomka, 1930s) • Impacts provoked cardiac arrhythmia. • almost always induced by extra-systoles. • Ventricular fibrillation • Caused sudden death occurred in 20% of animals • These arrhythmias might be due to myocardial stretch which alter cellular electrophysiological properties
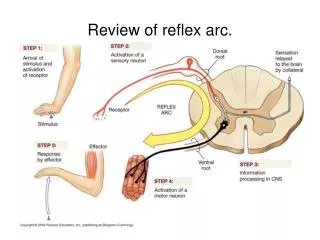
Escape beats Balloon Volume Mechano-electric Feedback Monophasic action potential (MAP) recording from the epicardial surface of a rabbit ventricle in response to volume pulses applied to a balloon inserted into the left ventricle.
Effects of Stretch • Depolarises cardiomyocyte during diastole • Stretch activated non-selective cation channels (Na+, Ca2+) • Shortens the action potential duration • Stretch activated K channels • Repolarises cardiomyocyte during systole. • Stretch activated K+ channels • Stretch activated non-selective cation channels (K+) • Decreases action potential amplitude ? (K+)
Decreased AP Amplitude 100 Decreased AP Duration Ca2+ Cross-over 50 Membrane Potential (mV) Na+ 0 Diastolic Depolarisation AP Prolongation K+ -50 -100 0 750 1500 Time (ms) Cardiac Action Potential - Stretch K+ Control K+ Stretch K+ Na+ & Ca2+ Na+ & Ca2+ Na+ & Ca2+
Frank Starling Mechanism • Greater diastolic volume results in an increase in cardiac performance • Heart responds to increases in mechanical stress by increasing the force of contraction and heart rate. • Thought to be due to mechanical alterations in myocyte. • Could MEF contribute ??? • We speculate that changes in the Action Potential could be altering contractility on a beat-to-beat basis.
Frank-Starling Relationship Contractility 0 25 Diastolic Pressure (mmHg)
Aims • To observe the effects of modulating SAC activity on Frank-Starling curve • Streptomycin (20 - 100 M, to block all SACs) • Gadolinium (1 - 20 M to block all SACs) • GsTx-4 (10 - 500 nM, to selectively block all SACs) • Chlorpromazine (0.1 - 1 M, to block SAPCs) • Chloroform (0.1 - 0.8 mM, to stimulate SAPCs) • Halothane ? (also stimulates SAPCs) • Relate changes in Frank-Starling curve to suggested activity of SACs.
Hypotheses • SACs are involved in the Frank-Starling curve, & thus in the beat-to-beat regulation of the heart. • SACs contribute to the shape or plateau of the Frank-Starling curve. • The Frank-Starling response is partly the result of changes in the cardiac action potential
Methods • Heart quickly excised from anaethesised male Sprague-Dawley Rat. • A latex balloon on a catheter, attached to a pressure transducer, is inserted via the left atrium into the left ventricle. • Volume of balloon adjusted in steps to produce 2.5 mmHg pressure changes
Methods • Varying concentrations of SAC blocking & stimulating agents will be circulated in the solution perfusing the heart. • Effect on agents on Frank-Starling mechanism analysed.
The pressure transducer monitors left ventricular pressure and the timing of balloon inflation. • Contact electrodes will record monophasic action potentials from the left left ventricle
2.5 mmHg Steps Systolic Diastolic -dV/dt dV/dt
Stabilisation period 50uM Streptomycin Soln Change (10 min) 100uM Streptomycin Pulse Pressure Soln Change Control Curves Re-Control Washout Final Curves (following washout) 20uM Streptomycin Rate of Contraction Phase I Protocol > 20 min Time (minutes)
Membrane Potential (mV) +20 0 -90 Action Potential Duration (ms) L-Type Ca2+ channel block - Gd 3+ - Streptomycin ? Expected Results stretch Increasing SAC Blocker Concentration Contractility 0 25 Diastolic Pressure (mmHg)
Preliminary Results Legend: Control 20M Strept Re-Control dP/dt (mmHg/second) 50M Strept 100M Strept Diastolic Pressure (mmHg)
Phase II Experiments Cardiac cycle-dependent contribution of SACs
Diagram of ventricular action potential showing the development of a secondary depolarisation during the terminal part of phase 3 (early afterdepolarisation, EAD) (A) and following repolarisation (delayed afterdepolarisation, DAD) (B). In each case when the amplitude of the EAD or DAD reaches threshold (fourth action potentials in each panel), it triggers a premature action potential. Diagram from Taggart and Sutton (1999).
Decreased AP Amplitude 100 Decreased AP Duration Ca2+ Cross-over 50 Membrane Potential (mV) Na+ 0 Delayed After Depolarisation AP Prolongation K+ -50 -100 0 750 1500 Time (ms) Cardiac Action Potential - Stretch K+ Control K+ Stretch K+ Na+ & Ca2+ Na+ & Ca2+ Na+ & Ca2+
Decreased AP Amplitude 100 Decreased AP Duration Cross-over 50 Early After Depolarisation Membrane Potential (mV) 0 -50 -100 0 750 1500 Time (ms) Cardiac Action Potential - Stretch Control Stretch Na+ & Ca2+
Unphysiological Stretch • If the myocardium is subjected to unphysiological amounts of stretch during the repolarisation phase of the action potential, depolarisations can occur. • Triggered activities arise when the magnitude of these depolarisations are sufficient to induce premature action potentials. • Triggered activities may result in runs of tachycardia or arrhythmia.
Aims (Part II) • To characterise cardiac cycle-dependent effects of stretch in the heart. • To determine the contribution of various SACs throughout the cardiac cycle.
Hypotheses • Non-selective SACs are most important during diastole • K+-selective SACs are more specifically involved in the early termination of the cardiac AP. • Both populations of SACs are important and their individual effects are cardiac phase-dependent (ie dependent on timing and the cardiac cycle).
0 Membrane Potential mV EAD -90 300ms Expected Results (Pt II) • Due to non-selective SACs • Blocked by: • Streptomycin • Gadolinium • GsTx-4
0 Membrane Potential mV DAD -90 Expected Results (Pt II) 300ms • Due to non-selective SACs • Blocked by: • Streptomycin • Gadolinium • GsTx-4
Early Termination 0 Membrane Potential mV -90 300ms Expected Results (Pt II) • Due to both non-selective and K+ selective SACs • Partially Blocked By • Streptomycin • Gadolinium • GsTx-4 • Chlorpromazine
Early Termination 0 Membrane Potential mV -90 300ms Expected Results (Pt II) • Due to both non-selective and K+ selective SACs • Partially Stimulated By • Chloroform • Halothane
Phase III Stretch-Activated Ion Channels in Human Atria
Effect of Stretch on Atrium • In humans, a change in the venous return had been found to affect heart rate. Donald and Shepherd (1978) reported that healthy volunteers who were required to remain in a supine position had an increase in heart rate when their legs were elevated. • SACs located within the sino-atrial node (SAN), are proposed to be involved in the positive chronotropic response of the heart to mechanical stress (Kohl, et. al., 1999)
The shorter the action potential duration, the earlier the subsequent action potential can be elicited. • As SACs activation can be involved in the shortening of APD, a patient with chronic atrial dilation would be more susceptible to re-entry arryhthmias.
Stretch-induced arrhythmia inhibited by Streptomycin & Gadolinium • Stretch-induced arrhythmia not inhibited by L-type / Na channel blockers • Verapamil, nifedipine, TTX
Non-selective SACs induce a depolarising current when activated during diastole while the TREK-1 current is hyperpolarising. Half-maximal activation of these cationic non-selective channels occur at 1.5mm Hg whereas for TREK-1, it occurs at a higher level of stretch, ie. around 12 mmHg (Terrenoire, et. al. 2001; Kim, 1992), suggesting that TREK-1 activation will occur secondary to the activation of these cationic non-selective SACs (Terrenoire, et al., 2001). Hence, TREK-1 channels could function as a negative feedback to the stretch-activated cationic non-selective channels.