Download
1 / 1
10 likes | 122 Vues
UNSCHEDULED ADMISSIONS AND DELIVERY IN WOMEN WITH PRIOR CAESAREAN BIRTH AND PLANNED FOR DELIVERY BY ELECTIVE CAESAREAN M Suchetha , R Jameison; Princess Royal Maternity Hospital ,Glasgow , United Kingdom.

E N D
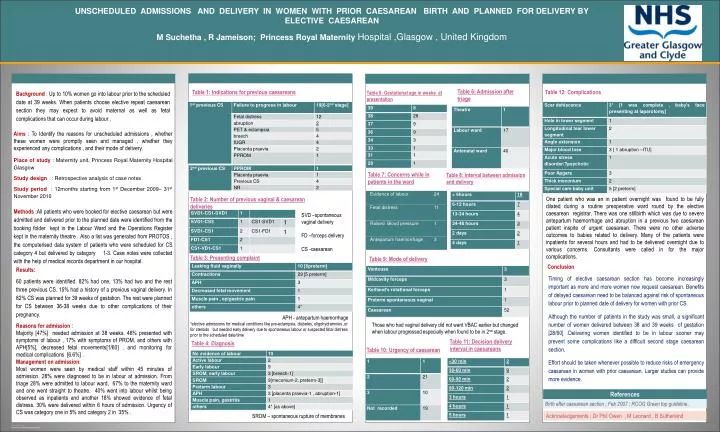
UNSCHEDULED ADMISSIONS AND DELIVERY IN WOMEN WITH PRIOR CAESAREAN BIRTH AND PLANNED FOR DELIVERY BY ELECTIVE CAESAREAN M Suchetha , R Jameison; Princess Royal Maternity Hospital ,Glasgow , United Kingdom Background : Up to 10% women go into labour prior to the scheduled date at 39 weeks. When patients choose elective repeat caesarean section they may expect to avoid maternal as well as fetal complications that can occur during labour . Table 6: Admission after triage Table 1: Indications for previous caesareans Table 12: Complications Table 5: Gestational age in weeks at presentation Aims : To Identify the reasons for unscheduled admissions , whether these women were promptly seen and managed , whether they experienced any complications , and their mode of delivery. Place of study : Maternity unit, Princess Royal Maternity Hospital Glasgow Study design : Retrospective analysis of case notes Study period : 12months starting from 1st December 2009– 31st November 2010 Table 7: Concerns while in patients in the ward Table 8: Interval between admission and delivery One patient who was an in patient overnight was found to be fully dilated during a routine preoperative ward round by the elective caesarean registrar. There was one stillbirth which was due to severe antepartum haemorrhage and abruption in a previous two caesarean patient inspite of urgent caesarean. There were no other adverse outcomes to babies related to delivery. Many of the patients were inpatients for several hours and had to be delivered overnight due to various concerns. Consultants were called in for the major complications. Table 2: Number of previous vaginal & caesarean deliveries Methods :All patients who were booked for elective caesarean but were admitted and delivered prior to the planned date were identified from the booking folder kept in the Labour Ward and the Operations Register kept in the maternity theatre . Also a list was generated from PROTOS , the computerised data system of patients who were scheduled for CS category 4 but delivered by category 1-3. Case notes were collected with the help of medical records department in our hospital. SVD –spontaneous vaginal delivery FD –forceps delivery CS -caesarean Table 3: Presenting complaint Table 9: Mode of delivery Results: 60 patients were identified. 82% had one, 13% had two and the rest three previous CS. 15% had a history of a previous vaginal delivery. In 82% CS was planned for 39 weeks of gestation. The rest were planned for CS between 36-38 weeks due to other complications of their pregnancy. Reasons for admission : Majority [47%] needed admission at 38 weeks. 48% presented with symptoms of labour , 17% with symptoms of PROM, and others with APH[5%], decreased fetal movements[1/60] , and monitoring for medical complications [6.6%] . Management on admission: Most women were seen by medical staff within 45 minutes of admission. 28% were diagnosed to be in labour at admission. From triage 28% were admitted to labour ward, 67% to the maternity ward and one went straight to theatre. 40% went into labour whilst being observed as inpatients and another 18% showed evidence of fetal distress. 30% were delivered within 6 hours of admission. Urgency of CS was category one in 5% and category 2 in 35% . Conclusion Timing of elective caesarean section has become increasingly important as more and more women now request caesarean. Benefits of delayed caesarean need to be balanced against risk of spontaneous labour prior to planned date of delivery for women with prior CS. Although the number of patients in the study was small, a significant number of women delivered between 38 and 39 weeks of gestation [28/60] .Delivering women identified to be in labour sooner may prevent some complications like a difficult second stage caesarean section. Effort should be taken whenever possible to reduce risks of emergency caesarean in women with prior caesarean. Larger studies can provide more evidence. APH - antepartum haemorrhage *elective admissions for medical conditions like pre-eclampsia, diabetes, oligohydramnios ,or for steroids but needed early delivery due to spontaneous labour or suspected fetal distress prior to the scheduled date/time Those who had vaginal delivery did not want VBAC earlier but changed when labour progressed especially when found to be in 2nd stage. Table 11: Decision delivery interval in caesareans Table 4: Diagnosis Table 10: Urgency of caesarean References Birth after caesarean section , Feb 2007 ; RCOG Green top guideline. Acknowledgements : Dr Phil Owen , M Leonard , B Sutherland SROM – spontaneous rupture of membranes