Download
1 / 71
720 likes | 904 Vues
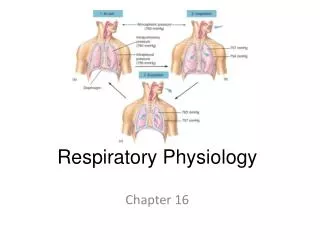
Respiratory physiology. Respiration is the process by which the body takes in and utilizes oxygen (O 2 ) and gets rid of carbon dioxide (CO 2 ). Respiration can be divided into four major functional events. Ventilation : Movement of air into and out of lungs

E N D
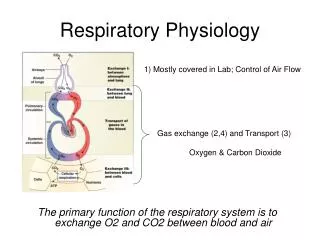
Respiration is the process by which the body takes in and utilizes oxygen (O2) and gets rid of carbon dioxide (CO2).
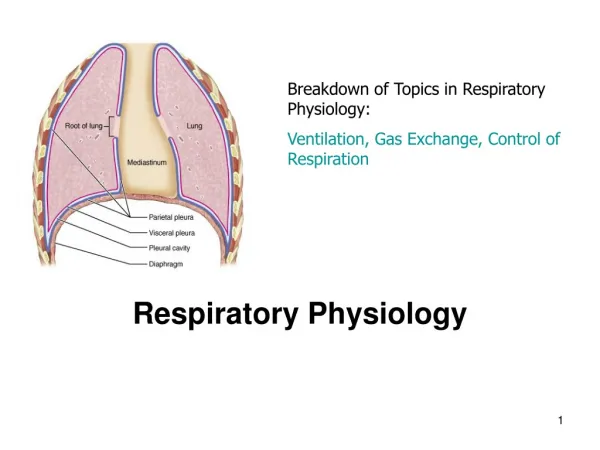
Respiration can be divided into four major functional events • Ventilation: Movement of air into and out of lungs • Gas exchange between air in lungs and blood • Transportof oxygen and carbon dioxide in the blood • Internal respiration: Gas exchange between the blood and tissues
Respiratory System Functions • Gas exchange: Oxygen enters blood and carbon dioxide leaves • Regulation of blood pH: Altered by changing blood carbon dioxide levels • Voice production: Movement of air past vocal folds makes sound and speech • Olfaction: Smell occurs when airborne molecules drawn into nasal cavity • Protection: Against microorganisms by preventing entry and removing them
Section 1 Pulmonary Ventilation Pulmonary ventilation means the inflow and outflow of air between the atmosphere and the lung alveoli, which is determined by the activity of the airways, the alveolus and the thoracic cage.
Respiratory System Divisions • Upper tract • Nose, pharynx and associated structures • Lower tract • Larynx, trachea, bronchi, lungs
Conducting Zone • All the structures air passes through before reaching the respiratory zone. • Cartilage holds tube system open and smooth muscle controls tube diameter • Warms and humidifies inspired air. • Filters and cleans: Insert fig. 16.5
Respiratory Zone • Region of gas exchange between air and blood. • Includes respiratory bronchioles and alveolar sacs.
Bronchioles and Alveoli
Breathing • Occurs because the thoracic cavity changes volume • Insipiration uses external intercostals and diaphragm • Expiration is passive at rest, but uses internal intercostals and abdominals during severe respiratory load • Breathing rate is 10-20 breaths / minute at rest, 40 - 45 at maximum exercise in adults
Pleural fluid produced by pleural membranes • Acts as lubricant • Helps hold parietal and visceral pleural membranes together
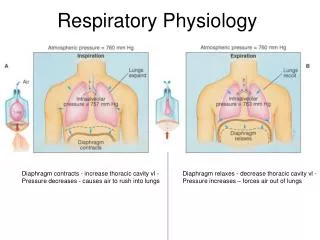
Ventilation • Movement of air into and out of lungs • Air moves from area of higher pressure to area of lower pressure • Pressure is inversely related to volume
Conducting Airways Lungs Gas Exchange Pleural Cavity Very small space Maintained at negative pressure Transmits pressure changes Allows lung and ribs to slide Chest Wall (muscle, ribs) Diaphragm (muscle) Pleural CavityImaginary Space between Lungs and chest wall Principles of Breathing Functional Unit: Chest Wall and Lung Follows Boyle’s Law:Pressure (P) x Volume (V) = Constant
CW Principle of Breathing Follows Boyle’s Law: PV= C At Rest with mouth open Pb = Pi = 0 Pb Airway Open A Pi PS D 1
Principle of Breathing Follows Boyle’s Law: PV= C • At Rest with mouth open Pb = Pi = 0 • Inhalation: • Increase Volume of Rib cage • Decrease the pleural cavity pressure- Decrease in Pressure inside (Pi) lungs Pb Airway Open A Pi PS CW D 2
Principle of Breathing Follows Boyle’s Law: PV= C • At Rest with mouth open Pb = Pi = 0 • Inhalation: • Pb outside is now greater than Pi- Air flows down pressure gradient • Until Pi = Pb Pb Airway Open A Pi CW PS D 3
Principle of Breathing Follows Boyle’s Law: PV= C • At Rest with mouth open Pb = Pi = 0 • Exhalation: Opposite Process • Decrease Rib Cage Volume Pb Airway Open A Pi CW PS D 4
Principle of Breathing Follows Boyle’s Law: PV= C • At Rest with mouth open Pb = Pi = 0 • Exhalation: Opposite Process • Decrease Rib Cage Volume • Increase in pleural cavity pressure - Increase Pi Pb Airway Open A Pi CW PS D 5
Principle of Breathing Follows Boyle’s Law: PV= C • At Rest with mouth open Pb = Pi = 0 • Exhalation: Opposite Process • Decrease Rib Cage Volume • Increase Pi • Pi is greater than Pb • Air flows down pressure gradient • Until Pi = Pb again Pb Airway Open A Pi CW PS D 6
Rib Cage Contract IntercostalsContractto Lift Spine Rib Diaphragm Volume Volume Ribs Mechanisms of Breathing: How do we change the volume of the rib cage ? • To Inhale is an ACTIVE process • Diaphragm • External Intercostal Muscles Both actions occur simultaneously – otherwise not effective
II Respiratory Resistance Including Elastic Resistance and Inelastic resistance
Elastic Resistance A lung may be considered as an elastic sac. The thoracic wall also can be considered as an elastic element. So during inspiration the inspiratory muscles must expand the thoracic cage which are together with the elastic resistance.
Elasticity • Tendency to return to initial size after distension. • High content of elastin proteins. • Very elastic and resist distension. • Recoil ability. • Elastic tension increases during inspiration and is reduced by recoil during expiration.
Compliance • Distensibility (stretchability): • Ease with which the lungs can expand. • The compliance is inversely proportional to elastic resistance • Change in lung volume per change in transpulmonary pressure. • DV/DP • 100 x more distensible than a balloon.
Static lung compliance C = DV/DP 100 deflation Lung volume (%TLC) 50 normal breathing inflation 0 0 30 Transpulmonary pressure (cmH2O)
The elastic forces can be divided into two parts: • the elastic forces of the lung tissue itself • 2) the elastic forces caused by surface tension of the fluid that lines the inside wall of the alveoli. • The elastic forces caused by surface tension are much more complex. Surface tension accounts for about two thirds of the total elastic forces in a normal lungs.
Surface Tension • Force exerted by fluid in alveoli to resist distension • Lungs secrete and absorb fluid, leaving a very thin film of fluid. • This film of fluid causes surface tension.. • H20 molecules at the surface are attracted to other H20 molecules by attractive forces. • Force is directed inward, raising pressure in alveoli.
At surface Unbalanced forces Generate Tension Within Fluid All forces balance What is Surface Tension ?
Surface Tension • Law of Laplace: • Pressure in alveoli is directly proportional to surface tension; and inversely proportional to radius of alveoli. • Pressure in smaller alveolus would be greater than in larger alveolus, if surface tension were the same in both. Insert fig. 16.11
AirFlow Expand Collapse Effect of Surface Tension on Alveoli size
Surfactant • Phospholipid produced by alveolar type II cells. • Lowers surface tension. • Reduces attractive forces of hydrogen bonding by becoming interspersed between H20 molecules. • Surface tension in alveoli is reduced. • As alveoli radius decreases, surfactant’s ability to lower surface tension increases.
Low S/unit Area Slider - Change Surface Area Increase Area DecreaseArea Surfactant High S/unit Area Area Saline Saline Tension Area dependence of Surfactant action
Factors Contributing to Compliance - Hysteresis Normal (with surfactant) Saline Filled Volume L 6 3 Without surfactant RV 0 Pleural Pressure - 30 cm H2O 0 - 15
Inelastic Resistance The inelastic resistance comprises the airway resistance (friction) and pulmonary tissue resistance (viscosity, and inertia). Of these the airway resistance is by far the more important both in health and disease. It account for 80%-90% of the inelastic resistance.
Airway Resistance • Airway resistance is the resistance to flow of air in the airways and is due to : • 1) internal friction between gas molecules • 2) friction between gas molecules and the walls of the airways
Laminar flow • … is when concentric layers of gas flow parallel to the wall of the tube. The velocity profile obeys Poiseuille’s Law (pg 43:11)
Poiseuille and Resistance • Airway Radius or diameter is KEY. • radius by 1/2 resistance by 16 FOLD - think bronchodilator here!!
Airway resistance increase • Any factor that decreases airway diameter, or increases turbulence will increase airway resistance, eg: • Rapid breathing: because air velocity and hence turbulence increases • Narrowing airways as in asthma, parasympathetic stimulation, etc. • Emphysema, which decreases small airway diameter during forced expiration
Control of Airway Smooth Muscle • Neural control • Adrenergic beta receptors causing dilatation • Parasympathetic-muscarinic receptors causing constriction • NANC nerves (non-adrenergic, non-cholinergic) • Inhibitory release VIP and NO bronchodilitation • Stimulatory bronchoconstriction, mucous secretion, vascular hyperpermeability, cough, vasodilation “neurogenic inflammation”