
overview of psoriasis
E N D
Presentation Transcript
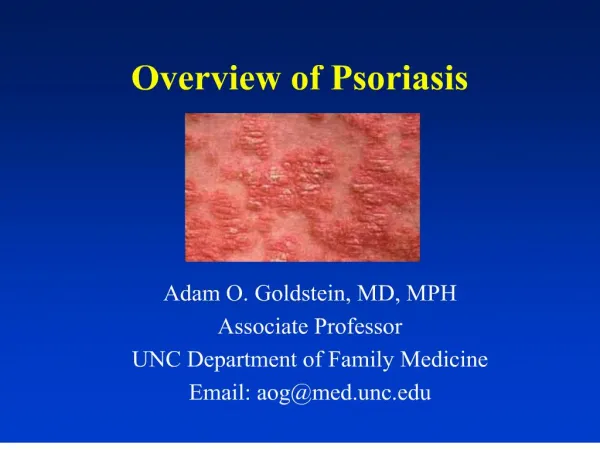
1. Overview of Psoriasis Adam O. Goldstein, MD, MPH
Associate Professor
UNC Department of Family Medicine
Email: aog@med.unc.edu
2. Objectives 1. Differentiate psoriasis types
2. Form differential dx
3. Review tx guidelines
4. Review new products
5. Learn 2 additional patient education pearls
3. �I am silvery, scaly. Puddles of flakes form wherever I rest my flesh.... Lusty, though we are loathsome to love. Keen-sighted, though we hate to look upon ourselves. The name of the disease, spiritually speaking, is�.
4. Psoriasis: Incidence 2-3% U.S. (6.4 million)
200,000 new cases/year
300,000 have >20% BSA
Median age dx: 30
Two peaks: 16-22, 57-60
Costs: $2 billion/year
Mean per patient costs $3000 Psoriasis is a chronic inflammatory skin disease characterized
by thick, raised lesions. Approximately 6.4 million people in the U.S. suffer from
psoriasis. Historically, between 150,000 and 260,000 new cases are diagnosed
each year in the U.S. It has been estimated that the annual cost of psoriasis
outpatient care in the U.S. is between US$1.6 billion and US$3.2 billion, with an
average annual cost per patient estimated between US$1,400 and US$6,700. At
present, no known cure exists for psoriasis and current therapies have unsatisfactory
efficacy and potentially unacceptable side effects.Psoriasis is a chronic inflammatory skin disease characterized
by thick, raised lesions. Approximately 6.4 million people in the U.S. suffer from
psoriasis. Historically, between 150,000 and 260,000 new cases are diagnosed
each year in the U.S. It has been estimated that the annual cost of psoriasis
outpatient care in the U.S. is between US$1.6 billion and US$3.2 billion, with an
average annual cost per patient estimated between US$1,400 and US$6,700. At
present, no known cure exists for psoriasis and current therapies have unsatisfactory
efficacy and potentially unacceptable side effects.
5. Psoriasis: Quality of Life 50% seek treatment
As debilitating as other chronic illnesses
> rates depression & alcohol abuse
(Sharma, J Dermatol, 2001)
6. Case Bob- 34 yo insurance executive
history of psoriasis for 8 years
scalp, elbows, knees and trunk
Got topical steroid (Psorcon E, 60 gms) from dermatologist 3 years ago
helped with itching
Wants a renewal and wonders if needs to see a dermatologist
You estimate 5-10% involvement of skin with plaque psoriasis
7. Case What is your treatment plan?
Do you refer him to a dermatologist?
8. Psoriasis: Definition
Chronic, remitting and relapsing
Scaly and inflammatory
Genetically influenced
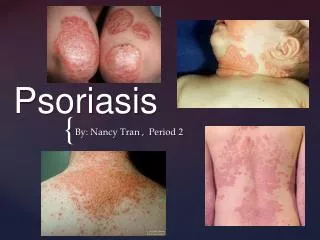
9. Psoriasis: Morphology: Circumscribed, thickened, plaques with secondary erythema and thick, silvery scales
10. Psoriasis: Pathogenesis Hyperproliferation of the epidermis
Normal skin cell matures in 28-30 days
Psoriatic skin cell matures in 3-6 days
11. Psoriasis: Types Plaque-typeLocalized or Generalized
PustularLocalized or Generalized
12. Psoriasis Arthritis associated (5-7%)
13. Psoriasis: Distribution
(From Pardasan AG, et al. Am Fam Physician 2000)
14. Psoriasis: Distribution Extensor
15. Psoriasis: Distribution Extensor
16. Psoriasis: Distribution Nails
17. Psoriasis: Distribution Genitalia
18. Psoriasis: Distribution Hands & feet
19. Psoriasis: Distribution Pustular
20. Psoriasis: Distribution Intertriginous/inverse- armpits, groin, under breasts (less thick �silvery�scale)
21. Psoriasis: Distribution Guttate-small red dots (Gutta = drops)
Appears suddenly after a strep, URI, other infection, stress, medications
22. Psoriasis: Guttate Appears after strep, URI, stress, medica-tions
23. Psoriasis: Distribution Erythrodermic
Widespread erythema, itching, pain, edema
25. Psoriasis: Distribution Sites of trauma (Koebner�s phenomenon)
26. Psoriasis: Diagnosis Early on, may look like other diseases
Bx may be necessary
27. Psoriasis: Differential Diagnosis Drug eruption
28. Psoriasis: Differential Diagnosis secondary syphilis
29. Psoriasis: Differential Diagnosis Seborrhea: Finer scale, central facial, scalp, central chest; Greasier; Sebopsoriasis
30. Psoriasis: Differential Diagnosis dermatophyte infections (Tinea)
KOH negative
scale not as thick or silvery
31. Psoriasis: Differential Dx intertriginous: diaper dermatitis/candidiasis
satellite pustules, beefy red, maceration; KOH positive for yeast in candidiasis; may coexist
32. Psoriasis: Differential Diagnosis Eczema
Neuro-dermatitis/ lichen simplex chronicus
33. Psoriasis: Differential Dx lichen planus
34. Psoriasis: Differential Diagnosis lupus erythematosus
35. Psoriasis: Differential Diagnosis pityriasis rosea
36. Psoriasis: Differential Diagnosis Cutaneous T-cell lymphoma
37. Psoriasis: Principals of Treatment Individualize treatment based on:
self-image, symptoms, interference with social interactions, expectations & scientific evidence
Patient education: Control, not cure
Pearl:
Combine products for better long-term control and fewer SE�s
38. Psoriasis: Treatment Flares
skin injury (including dryness, scratching)
sunburn
infections (strep, HIV)
psychological stress
medications
39. Psoriasis: Treatment Medications linked to psoriatic flares:
Lithium
Beta blockers
ACE inhibitors
Antimalarials
Indomethacin
40. Psoriasis Pearl Avoid systemic corticosteroids
41. Psoriasis: Treatment <5% sunlight + topical tx
5-20% sunlight + topical tx +/- systemic
>20% systemic tx +/- light therapy
42. Psoriasis: Treatment Sunlight
43. No good evidence that non-drug tx�s work
Topical tx�s effective in short-term (few comparative RCT�s)
RCT�s show UVB and PUVA effective short/long term (long term risk PUVA-SCCa)
Cyclosporin clears short term but toxic
44. Psoriasis: < 20% BSATopical Therapies 1. Emollients
2. Keratolytic agents
3. Topical steroids
4. Calcipotriene
5. Tazarotene gel
6. Topical calcineurin inhibitors
7. Anthralin
8. Coal tar
( BMJ 2001)
45. 1. Emollient cleansers and lotions/cream
Mild cleansers
Moisturizers
46. 2. Keratolytic Agents WHEN THE SCALE IS REALLY THICK
Scalp: P & S liquid
Body: 2-10% salicylic acid qd- bid
47. Never treated-
start medium potency
follow up in 2 weeks
Previously treated
start high potency
2-4 weeks, then taper
Always use lower potencies on face and intertriginous areas
48. Creams most body parts
Lotions/mousse hairy areas
Ultrapotent/potent BID 2-3 weeks to thick lesions
Taper to weekend use only or:
Taper to Class III for maintenance to avoid atrophy/striae
Educate on:
�tolerance�, signs of atrophy, tapering & relapse
If topical steroids insufficient:
Steroids + occlusion (plastic wrap QHS- if no atrophy)
Steroids + calcipotriene cream/ointment or tazarotene gel
Coal tar products and/or Anthralin
(Tristani-Firouzi, Cutis, 1998)
49. Intralesional injections Isolated recalcitrant lesions
TAC 3-10mg/cc
in NS to plaques < 3 cm
50. 4. Calcipotriene 0.005% (cream, ointment, solution) Calcipotriene (Dovonex)
simulates differentiation
inhibits proliferation
> effective as steroids, tar, anthralin
> irritation than steroids
Use cautiously if renal or calcium-related conditions, especially (< 60 gm/week)
Use > 4 wks to determine effectiveness
51. 4. Calcipotriene 0.005% Use with potent topical corticosteroid (halobetasol) BID x 2-4 weeks
less potent topical corticosteroids for facial or groin use
may apply simultaneously
Continue calcipotriene use BID and taper corticosteroid use to weekends only
Helps prevent rebound flares
Helps avoid atrophy
Taper off steroid first, then calcipotriene
(Koo, Skin & Aging 2002)
52. 5. Tazarotene Topical Gel/ Cream Tazarotene (Tazorac)
Mechanism of action not well defined
Vitamin A derived
Inhibits cornified envelope formation
Suppresses inflammation in the epidermis
53. 5. Tazarotene Topical Gel (0.05-0.1% ) Use with medium- high potency topical steroids QD-BID and Tazarotene gel QHS
(63% post-treat flare with steroids alone vs 14% steroids + tazarotene)
After 2-4 weeks, gradually decrease potent topical steroids to weekend use only
Continue or slowly taper tazarotene gel
(Koo, J Am Acad Dermatol 2000)
54. 5. Tazarotene Topical Gel/Cream Educate
apply very small amount to center of plaques
initial increased erythema and scaling
confine application to plaques
do not �chase� erythema
Pregnancy = Do not use
Use for > 4-6 weeks before discontinuing
55. 6. Steroid Sparing Topical calcineurin inhibitors
Tacrolimus ointment & Pimecrolimus cream
Facial and intertriginous areas
(Freeman, J Am Acad Dermatol, 2003)
56. Tacrolimus ointment & Pimecrolimus cream Safety?
In 2005, FDA warnings about possible link between topical calcineurin inhibitors and cancer (? inc risk of lymphoma and skin cancers)
No definite causal relationship �� �
FDA recommends these agents only as second-line therapy in patients unresponsive to or intolerant of other treatments
Use for short periods of time and minimum amount
Avoid continuous use
57. 7. Anthralin Antimitotic & reducing agent
Short-contact therapy
Creams:
Drithocreme 0.1%,0.25%,0.5%, 1%
Micanol 1%*
Psoriatec 1%
Ointment
Anthraderm 0.1%,0.25%,0.5%, 1%
* Micanol does not stain skin if rinsed with cool to lukewarm water
Use daily until skin is smooth (2-4 weeks)
(Koo, Skin & Aging, 2002)
58. 8. Coal Tar Useful as an antimitotic agent
Folliculitis, Staining, Photosensitizer, Smell
Dozens of products
59. Algorithm for Treatment of Localized Psoriasis
60. Scalp Psoriasis Medicated shampoos 5-10 minutes daily
keratolytics (salicylic acid)
coal tar based
Topical steroids in lotion or solution form
Class I to II lotion or scalp application, tapering to:
Class III lotion, solution, oil
Calcipotriene solution
Use qhs in addition to topical corticosteroids
61. Scalp Psoriasis Topical corticosteroids in mousse
BMV foam (Luxiq)-may be used on nonfacial/genital areas
Used qd-bid, less often with improvement
Foam superior efficacy & preferred by patients compared with lotion
62. Genital Psoriasis Mid potency steroids can be use cautiously and for limited time
short-term mometasone
Reduce to low-potency creams asap
desonide cream
Consider compounding hydrocortisone 2.5% cream and ketoconazole (Nizoral) cream ,
Cautious use of calcipotriene
Cautious use of anthralin
(Lebwoh, J Am Acad Dermatol 2001)
63. Nail Psoriasis topical fluorouracil qhs
tazarotene gel 0.1% qhs
class I-II topical steroids
posterior nailfold intralesional Kenalog 5-10 mg/cc
methotrexate
64. Topical Treatments GIVE ENOUGH WITH REFILLS!
BE AWARE OF $$$$!
65. Generalized plaque-type psoriasis >20% BSA Ultraviolet light: UVB or PUVA (oxpsoralens photosensitizer + UVA)
Methotrexate
Retinoids: Acitretin/ Etretinate
Sulfasalazine
Cylclosporine
66. Ultraviolet light: UVB Indications:
guttate psoriasis
>20% BSA involved
unresponsive to topical therapies
Most effective wavelength of light for psoriasis (280-320 nm)
narrow band UVB (new)
not found in high enough concentrations in tanning salons
natural sunlight
67. Ultraviolet light: UVB Risks: burns, especially corneal, conjunctivitis (Face can be shielded)
Very little toxicity involved
Home light therapy
Eximer laser
68. Ultraviolet light: PUVA Indications:
severe or incapacitating psoriasis
previous failure of conventional topical therapy
previous failure of UVB therapy
rapid relapse after the above forms of therapy
Must be administered in dermatologist office
69. Ultraviolet light: PUVA Contraindications:
photosensitive diseases
photosensitive drugs
previous or present skin cancers
previous x-ray therapy to the skin
cataracts
pregnancy
70. Ultraviolet light: PUVA Increased risk of squamous cell carcinoma
Possible increased risk of melanoma (controversial)
Photoaging
71. Methotrexate Indications:
psoriatic erythroderma
acute pustular psoriasis
localized pustular psoriasis
psoriatic arthritis
extensive psoriasis unresponsive to other, less toxic therapies
psoriasis in areas preventing the individual from obtaining gainful employment
psoriasis that is psychologically disabling
72. Methotrexate Contraindications:
pregnancy
history of significant liver disease
excessive alcohol intake
abnormal liver function
poor renal function
leukopenia
active peptic ulcer
active, severe infectious disease
unreliable patient
73. Methotrexate Test dose 2.5-5.0 mg once
Dosage 10-25 mg 1X/Week
Baseline labs: (cbc w/platelets, urinalysis, BUN, creatinine, liver functions, CXR)
Ongoing:
liver biopsy (0.5-1.5 grams)
wbc and PLT q wk x 4 weeks; 6 days after last dose
Hct, liver functions, urinalysis, serum creatinine every 3 months, at least 6 days after last dose
Folic Acid 1-5 mg/day for nausea
74. Acitretin (Soriatane) New retinoid with shorter half-life than etretinate
10, 25 mg capsules
Particularly useful in combination with light therapy
Many potential side effects
hepatotoxicity
elevation of triglycerides
dry eyes
hyperostosis
teratogenic
75. Biologics Alefacet Amevive
Efalizumab Raptiva
Etanercept Enbrel
Infliximab Remicade
ximab = chimeric monoclonal antibody
zumab = humized monoclonal antibody
umab= human monoclonal antibody
cept = receptor-antibody fusion protein
76. Emerging Therapies Oral Pimecrolimus
77. Alternative Therapies Fish oil
Aloe vera
Oral Vit. D
Stress reduction
Lifestyle change
Antistrep tx
Thermal bath
Acupuncture
78. Alternative Therapies
79. Alternative Therapies
80. Case Treatment plan:
82. Psoriasis: Patient Education National Psoriasis Foundation, 6600 S. W. 92nd Avenue, Suite 300, Portland, OR 97223, 503-244-7404, Fax. 503-245-0626
http://www.psoriasis.org/
Patient ed brochure
http://www.aafp.org/afp/20000201/20000201d.html
Comprehensive WEB listing
http://www.edae.gr/psoriasis.html
84. Bibliography Bruner CR, et al. A systematic review of adverse effects associated with topical treatments for psoriasis. Dermatol Online J 2003; 9(1): 2.
Lebwohl MG, Tan MH, Meador SL, Singer G. Limited application of fluticasone proprionate ointment, 0.005% in patients with psoriasis of the face and intertriginous area. J Am Acad Dermatol 2001; 44: 77-82.
Koo JY, Lowe NJ, Lew-Kaya DA, et al. Tazarotene plus UVB phototherapy in the treatment of psoriasis. J Am Acad Dermatol 2000; 43: 821-8.
Tausk F, Whitmore SE. A pilot study of hypnosis in the treatment of patients with psoriasis. Psychotherapy & Psychosomatics 1999; 68: 221-5.
Tristani-Firouzi P, Krueger GG. Efficacy and safety of treatment modalities for psoriasis. Cutis 1998; 61S: 11-21.
Jerner B, Skogh M, Vahlquist A. A controlled trial of acupuncture in psoriasis: no convincing effect. Acta Dermato-Venereol 1997; 77: 154-6.
Syed TA, Ahmad SA, Holt AH, et al. Management of psoriasis with Aloe vera extract in a hydrophilic cream: a placebo-controlled, double-blind study. Trop Med Internat Health 1996; 1: 505-9.
American Academy of Dermatology. Committee on Guidelines of Care, Task Force on Psoriasis. Guidelines of care for psoriasis. J Am Acad Dermatol 1993; 28: 632-7.
85. Gaston L, Crombez JC, Lassonde M, Bernier-Buzzanga J, Hodgins S. Psychological stress and psoriasis: experimental and prospective correlational studies. Acta Dermato-Venereol 1991; 156S: 37-43.
Fleischer AB Jr, Feldman SR, Rapp SR, et al. Alternative therapies commonly used within a population of patients with psoriasis. Cutis 1996; 58: 216-20.
Federman DG, Froelich CW, Kirsner RS. Topical psoriasis therapy. Amer Fam Physician 1999; 59: 957-62, 964.
Roenigk HH Jr, Auerbach R, Maibach H, Weinstein G, Lebwohl M. Methotrexate in psoriasis: consensus conference. J Am Acad Dermatol 1998; 38: 478-85.
Owen CM, Chalmers RJG, O'Sullivan T, Griffiths CEM. Antistreptococcal interventions for guttate and chronicplaque psoriasis. Cochrane Database of Systematic Reviews. Issue 1, 2001.
Pardasan AG, Feldman SR, Clark AR. Treatment of Psoriasis: An Algorithm-Based Approach for Primary Care Physicians. Am Fam Physician 2000; 61:725-733.
Sharma N, Koranne RV, Singh RK. Psychiatric morbidity in psoriasis and vitiligo: a comparative study. J Dermatol 2001; 28: 419-23.
Koo JY, Nguyen KD. Treating psoriasis patients: a topical therapy update. Skin and Aging 10: 35-39.
Van der Vleuten CJ. Management of scalp psoriasis: guidelines for corticosteroid use in combination treatment. Drugs 2001; 61(11): 1593-8.
Schon MP, Boehncke WH. Psoriasis. N Engl J Med 2005; 352: 1899-912 .