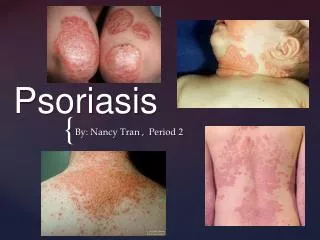
PSORIASIS
PSORIASIS. IDENTIFICATION AND MANAGEMENT. How can psoriasis present?. Plaques Flexural Guttate Scalp Hands and feet nails. Plaque psoriasis. Guttate psoriasis. Flexural psoriasis. Scalp psoriasis. Nail psoriasis. Hand and foot psoriasis. Management- Plaques.

PSORIASIS
E N D
Presentation Transcript
PSORIASIS IDENTIFICATION AND MANAGEMENT
How can psoriasis present? • Plaques • Flexural • Guttate • Scalp • Hands and feet • nails
Management- Plaques • Depends on amount of body surface affected. • Consider psychological impact and discuss • Emollient • Topical vitamin d analogue +/- moderately potent topical steroid short term. • Caution regarding Dovobet • Exorex for small multiple plaques • review
Plaque continued • Dithranol an option if motivated and able to apply correctly • Limited response- consider UVB • Systemic therapy- Methotrexate / Neotigason • Biological agents
Guttate psoriasis • May occur after a streptococcal throat infection • Often resolves after a few weeks • Topical tar e.g. Exorex • Mild topical steroid • Consider referral for UVB if not improving
Flexural Psoriasis • Often treated as thrush- look for clues • Milder vitamin d analogue( tacalcitol / calcitriol). Topical steroid ( clobetasone butyrate) • Reduce frequency when settled to maintain control
Scalp psoriasis • Challenging and requires dedication • Psoriasis association advice sheet explains how to apply treatments. • Mild - tar based shampoo used twice a week • Moderate - above+ calcipotriol or betamethasone scalp application 2-3 times a week • Severe – salicylic acid/ coal tar applied and left on overnight, comb out, wash then apply steroid/ vitamin d application.
Scalp cont’d • Maintain with 1-2 x a week vitamin d analogue or weakest topical steroid that will control + tar based shampoo.
Nail psoriasis • Exclude fungal infection- clippings • Nothing works topically. • Nail varnish for women
Hands and feet • Can be a challenge. • Emollient – thicker and possibly urea based • Salicylic acid to soften scale • Potent topical steroid – ointment/ occlusion • Vitamin d analogues bit impractical as need to apply a thick layer • Refer for PUVA and possibly systemic treatment
Pustular psoriasis • Does not mean infection
Useful sources of information • www.bad.org.uk • www.pcds.org.uk • www.psoriasis-association.org.uk • www.dermnet.org.nz • www.patient.co.uk