DOCUMENTING MEDICAL NECESSITY THRU OUTCOMES ASSESSMENT
710 likes | 1.34k Vues
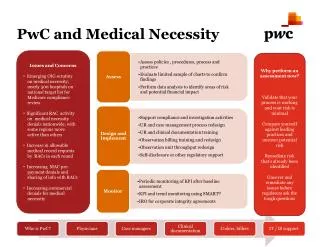
DOCUMENTING MEDICAL NECESSITY THRU OUTCOMES ASSESSMENT. OUTCOMES. Outcomes Assessment Collection and recording of information relative to health processes Outcomes Management Using information in a way that enhances patient care

DOCUMENTING MEDICAL NECESSITY THRU OUTCOMES ASSESSMENT
E N D
Presentation Transcript
OUTCOMES • Outcomes Assessment • Collection and recording of information relative to health processes • Outcomes Management • Using information in a way that enhances patient care (Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
The Era of Outcomes Assessment • Outcomes in clinical practice provide the mechanism by which the health care provider, the patient, the public, and the payer are able to assess the end results of care and its effect upon the health of the patient and society. • (Anderson & Weinstein, 1994).
Survival • To survive, in fact to flourish, in this era of accountability health care providers must be prepared to maintain and be able to provide appropriate documentation and patient records in a clinically efficient and economical manner. • (Hansen, 1994).
Health Policy • With the dawning, of the “era of accountability,” there are new social mandates directed toward health care providers and health-related facilities. Measurements of quality, satisfaction, efficacy, and effectiveness now serve as essential elements for health care decisions and matters of health policy. • (Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
Outcome Meanings • Health Care Customer - Meaning of Outcomes • Payers-purchasers Cost containment • Regulators HCP compliance • Administrators Efficiency-low utilization • Clinical Researchers Proof of a premise • Outcomes Experts Patient’s benefit • Health Care Providers Clinical-Health Status • (Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
Outcomes Criteria • Utility Is it useful? • Reliability Is it dependable? • Validity Does it do what it is supposed to? • Sensitivity Can it identify patients with a condition? • Specificity Can it identify those that do not have the condition? • Responsiveness Can it measure differences over time?
Outcome Measures Appropriate for Clinical Use • Questionnaires • General health status • Pain • Functional status • Patient satisfaction • Physiological outcomes • Utilization measures • Cost measures
Outcomes Measures Appropriately Used • When outcome measures are appropriately used and integrated into an evidence-based, patient-centered model of practice, there is accountability and quality assurance. • (Hansen DT, Mior S, Mootz RD in Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000)
Subjective Questionnaires • Subjective outcomes assessment information is gathered by the patient in self-administered questionnaires and scored by either the: • health care provider • staff members or • by a computer.
Subjective Questionnaires • In spite of the definition associated with the term “subjective,” these “pen-and-paper tools” have been described as very valid and reliable – in many cases more so than many of the “objective’ tests that health care providers have relied upon for years. • (Chapman-Smith, 1992; Hansen, 1994; Mootz, 1994).
Subjective vs Objective • It must be emphasized that although the term “subjective” carries negative connotations, the reliability/validity data published regarding these methods of collecting outcomes is exceptional, typically out-performing the test-retest reliability and validity of most “objective” physical performance tests. • (Chapman-Smith, 1992).
Subjective (Patient Driven) General Health Pain Perception Condition or Disease Specific Psychometric Disability Prediction Patient Satisfaction Objective (HCP Driven) Range of Motion Strength - Endurance Nonorganic Proprioception Cardiopulmonary Developmental Classification of Outcome Assessment Tools
Outcomes Assessment Tools • It is important to remember to utilize the same outcome assessment tool through the course of case management with each patient.
General Health Questionnaires (GHQ) • One can benefit from the use of a GHQ because it is not condition-specific and, therefore, can be applied to virtually any complaint. • Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000
Application of General Health Questionnaires (GHQ) • The application of a GHQ should, at minimum, be used at the following intervals: • At the time of the initial presentation for baseline establishment of outcomes assessment. • To identify problems for prompt management. • At a plateau in care or discharge for outcomes assessment of the treatment benefits or lack thereof. • Six months after discharge in order to evaluate the long-term benefits of treatment.
Normative Data - Rand 36General Health Questionnaire • Scale Normative - Exam 1 - Exam 2 • Health perception 72 46 66 • Physical functioning 84 42 78 • Role – Physical 81 0 59 • Role – Emotional 81 22 27 • Social functioning 83 55 70 • Bodily Pain 75 0 68 • Mental health 75 42 72 • Energy/fatigue 61 22 48 • Ware et al, 1993
Rand 36 – General Health Questionnaire • This can serve as a very practical reference tool to use for patient report of findings, to insurers to justify “medical necessity” for additional care, and to the health care provider to facilitate the decision making process of case management (referral, discharge).
Rand 36 Scales • Some of the scales – such as physical function, pain, and role (physical) of the RAND-36 are sensitive to change over time and parallel the patient’s symptomatology quite well.
Outcome-Based Practice • Correlating this information to the patient’s specific clinical data and then making a clinical decision based on the results represents a difficult but important step in making the “paradigm shift” into becoming an “outcome-based” practice. • Yeomans SG: The Clinical Application of Outcomes Assessment, Stamford Connecticut, Appleton & Lange, 2000
Pain Perception • Visual Analogue Scales • Reliable and valid (Jensen and Karoly, 1993). • Advantages over other measurement methods (Scott and Huskisson 1976, Price et al 1994).
Quadruple Visual Analogue Scale (QVAS) • Four specific factors - Von Korff et al, 1992 • CURRENT Pain Level • AVERAGE or TYPICAL Pain Level • Pain level at its BEST • Pain level at its WORST • Final Score • Ratings are averaged x 10 = TOTAL SCORE (Range 0 – 100)
QVAS – Guidelines • Chronic Patient • Average Pain = Last 6 months • Frequency • Every 2 weeks since a patient’s failure to progress over a 2-week period may indicate a need for a change in management approaches • (Haldeman et al, 1993).
Condition-specific • Over 40 low back functional questionnaires exist with five identified by researchers as “gold standards” (Kopec and Esdaile, 1995). • Sickness Impact Profile (Bergner et al, 1981) • Roland-Morris Disability Questionnaire (Roland and Morris, 1983) • Oswestry Low Back Pain Disability Questionnaire (Fairbank et al, 1980). • Million Visual Analogue Scale (Million et al, 1982). • Waddell Disability Index (Waddell, 1984).
Oswestry Questionnaire (Discharge Score) • A score of 11% may be used as an appropriate cut-off score for health care providers to consider for discharge and/or return to work in an uncomplicated Low Back Pain case. (Erhard et al 1994)
Revised Oswestry • Retitled section 8, now identified as “Social Life,” • This section was originally entitled “sex life” and was left blank quite often by respondents. • In the revised version, all ten sections are completed more often than in the original version. • Hudson-Cook N, Tomes-Nicholson K, Breen AC. A Revised Oswestry Back Disability Questionnaire. Manchester Univ Press, 1989.
Oswestry - Score Interpretation • 0-20% Minimal Disability • 20-40% Moderate Disability • 40-60% Severe Disability • 60-80% Crippled • 80-100% Bed Bound or Exaggerating
Oswestry Score – Statistically Significant Change (Minimal-Moderate Disability) • Initial Score - Change Necessary • 0-8 2 • 5-12 4 • 9-16 5 • 13-20 8 • 17-24 8 • Stratford et al, 1988
Roland-Morris Disability Questionnaire (RMQ) • Total Possible Score = 24. • “The best single study of assessing short-term outcomes of primary care patients with low back pain “(Von Korff and Saunders, 1996) • Scores greater than 13 = Significant disability associated with an unfavorable outcome • (Von Korff and Saunders, 1996) • Any change of less than 4 points is both too small to matter and too small to be reliable • (Stratford et al, 1996)
Neck Disability Inventory (NDI) • “was designed by modifying the Oswestry Low Back Pain Disability Questionnaire” • “The instrument was utilized on an initial sample of 17 consecutive patients with whiplash injuries with good statistical significance reported”.
Copenhagen Neck Functional Disability Scale (CNFDS) • “CNFDS demonstrates • short-term and day-to-day reliability • internal consistency • practicality • accurate patient perceptions regarding functional status and pain • doctor’s global assessment • responsiveness to change over long periods of time
CNFDS Score Range • Maximum point score is 30 and “indicates that the individual is extremely disabled because of neck trouble, whereas a score of 0 indicates that there is no neck trouble present.”
Headache Disability Inventory (HDI) • 25 question – condition specific often used in conjunction with the NDI for patients suffering from cervicogenic headaches (Jacobson et al, 1994) • 12 emotional questions • 13 functional questions
HDI Interpretation • 100 Points = Maximum possible Score • Headache Severity (Jacobson et al, 1994) • 2-32 = Mild • 33-59 = Moderate • 60 + = Severe • Positive Treatment Results • 29 point total score change (Jacobson et al, 1994)
Dizziness Handicap Inventory (DHI) • 25 questions evaluate the impact of vestibular system disease or dizziness on everyday life • Functional: 9 items • Emotional: 9 items • Physical: 7 items
DHI Studies • “good internal consistency, reliability, & validity demonstrated (Jacobson & Newman 1990). • “found to correlate with balance function tests that included electronystagmography, rotation testing, and platform posturography (Jacobson et al, 1991)
Tinnitus Handicap Inventory (THI) • 25 questions “developed to track patients who suffer from tinnitus pre- and post-treatment” (Newman 1996) • Functional: 12 items • Emotional: 8 items • Catastrophic: 5 items (identifies patients with psychosocial concerns) • “found to be valid, responsive, and easy to score and interpret.”
Temporomandibular Disorder Disability Index (TMD) • 10 questions and scored similar to Oswestry • “the tool has face-validity”
Spinal Stenosis Questionnaire • 18 items • Symptom Severity : 7 Items • Physical Function: 5 Items • Satisfaction: 6 Items
Spinal Stenosis Studies • “was found to be reproducible, valid, internally consistent, and responsive to clinical change in a geriatric spinal stenosis population pre and post-surgery” (Stucki et al, 1996). • This measure is meant to be used in conjunction with other existing spine and health status instruments.
Shoulder Injury Self-Assessment of Function • 15 item ADL tool included in the American Shoulder and Elbow Surgeons SEF (Barrett, 1987; Rowe, 1987) • 0 = Normal • 60 = Self-assessed Disabiltiy
Shoulder Pain and Disability Index (SPADI) • 13 point questionnaire measuring • Pain • Disability • Scale has been shown responsive to • Improved Change • Worsened Change
Elbow Performance Index • 100 point index (Morrey, 1993) • Pain - 45 points • Motion - 20 points • Stability - 10 points • Function - 25 points
Carpal Tunnel Syndrome Questionnaire (CTSQ) • “strength lies in its ability to track outcomes based on SYMPTOM SEVERITY and FUNCTION, which are two of the primary reasons presented to health care providers.” • 19 questions demonstrating “reproducibility, internal consistency, validity and responsiveness” • Symptom Severity: 11 items • Functional Status: 8 items
CTSQ Reproducibility and Consistency • “In comparing inter-rater agreement to objective measures, Levine et al point out the superior scores gathered by the CTSQ compared to the inter-rater agreement in ECG interpretation or between radiologists regarding the presence of osteoarthritis…” (Levine 1993)
CTSQ Measures • “this dispels the myth that so-called soft (subjective) outcomes such as the CTSQ are less valuable when compared to objective measures when, in fact, the subjective measures are often more sensitive, specific, and responsive than many objective measures.” (Koran, 1975)
CTSQ Validity • “CTSQ and traditional physical examination measures of median nerve function capture different but complementary outcome information. Therefore, symptom severity and functional status cannot be reliably compared to sensibility or nerve conduction testing.” (Levine et al, 1993)
Patient-Rated Wrist Evaluation • 150 point index • Pain - 50 points • Function • Specific Activities - 60 points • Usual Activities - 40 points
Hip Rating Questionnaire • 100 point index (Johanson et al, 1992) • Pain • Walking • Function • Arthritis
Patellofemoral Function Scale (PFS) • 8 item ADL tool “demonstrating potential to detect clinical change” (Reid, 1992) • 16 = Normal • 0 = Functional Disability