Pap Smear Guidelines Baylor College of Medicine Anoop Agrawal, M.D.
Pap Smear Guidelines Baylor College of Medicine Anoop Agrawal, M.D. Statistics. Cervical Cancer was once the #1 Cancer Killer of Women. Now Cervical Cancer Ranks #13 in the USA. An estimated 10,370 cases of invasive cervical cancer

Pap Smear Guidelines Baylor College of Medicine Anoop Agrawal, M.D.
E N D
Presentation Transcript
Pap Smear Guidelines Baylor College of Medicine Anoop Agrawal, M.D.
Statistics • Cervical Cancer was once the #1 Cancer Killer of Women • Now Cervical Cancer Ranks #13 in the USA • An estimated 10,370 cases of invasive cervical cancer • will be diagnosed, and 3,710 women will die from the disease • With the increase in pap smears, pre-invasive lesions are • detected much more frequently than invasive cancer. • Women with pre-invasive lesions have a 5 year survival rate of • nearly 100% • Those with cervical cancer detected early have a 5 year • survival rate of ~92%
Cervical Cancer and HPV • Between 93-100% of squamous cell cancer of the cervix • contains DNA from high risk types of HPV • HPV is transmitted via sexual activity • High risk HPV subtypes may lead to either low-grade or • high-grade intraepithelial lesions • High-grade lesions may progress to cervical cancer • However, most lesions are transient—they may result in no • signs at all or may become low-grade lesions
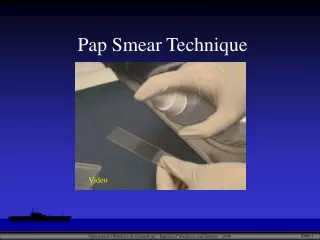
Pap Smears Purpose: 1) Detect cervical cancer at an early stage 2) Detect and remove high grade lesions and prevent potential cervical cancer • Sensitivity for high grade lesions = 70 – 80% • Limited by: • Small lesions • Inaccessible location • Poor sampling of lesion • Few abnormal cells on the slide • Small size of abnormal cells • Inflammation or Blood obscuring cell • visualization
Guidelines • ~50 % of cervical cancer diagnosed in the USA is found in • women who have never been screened • Another 10% occur in women who have not been screened for • 5 years • American Cancer Society and U.S. Preventative Services Task • Force have issued new guidelines regarding: • Timing of Initial Screening • Screening Intervals • Post-Hysterectomy Patients • When to End Screening
Both groups acknowledge that the greatest gains in reducing morbidity and mortality would likely involve increasing screening rates among women who are currently unscreened or screened only infrequently
When to Start Screening • Both Groups Recommend: • Begin Screening 3 years after the onset of sexual activity • Or • At age 21—whichevercomes first • Critical that adolescents who may not need yearly Pap smears • obtain other yearly preventative health care • Assessment of Health Risks • Contraception • Prevention Counseling • Screening and treatment of STDs
Rationale • Little risk of missing an important cervical lesion until • 3-5 years after the initial exposure to HPV • Earlier screening may result in over-diagnosis of cervical • lesions • These may regress spontaneously, but may lead to inappropriate • intervention • Young women who are infected with HIV and/or • immunocompromised should have Pap smears twice in the • first year after diagnosis and if normal—annually thereafter • In women age 13-22 most HPV infections are transient. 70% • of High-Risk HPV lesions regress in 3 years. 90% • regression for low-risk types. Regression is more • common in adolescents.
Screening Intervals • Once screening has begun, test annually until age 30 if using • conventional cytology or every 2 years if using liquid-based • cytology (ACS) • After age 30, if results are normal and study satisfactory for • 2-3 years in a row AND the patient has no new risk factors • OK to screen every 2 – 3 years thereafter • Studies suggest little added benefit of more frequent screening in • most women • Liquid-based cytology offers higher sensitivity than conventional • Pap smear with comparable specificity. • Liquid-based cytology costs $45 - $60, compared to $25 - $40 • for conventional Pap smear. If used at 3 year intervals, the • liquid-based cytology is cost-effective.
Screening Intervals • USPSTF recommends screening every 3 years based on limited evidence • ACOG recommends intiating screening with annual smears for 2 or 3 years; if these are negative, then intervals of up to 3 years. • ACOG identifies risk factors that might justify annual screening: • H/O Cervical Neoplasia • Known infections with HPV • Other STDs and HIV • High risk Sexual behavior • Chronic Corticosteroid Treatment
Rationale • More frequent screening increases sensitivity but also • increases unnecessary procedures and costs • Many of these lesions will resolve on their own
Post Hysterectomy Guidelines • Both sets of guidelines agree: • Should not continue to screen women who have had a • total hysterectomy for benign conditions • Presence of CIN 2/3 is not benign • Should continue to screen the small number of women who • retain their cervix • Women with h/o CIN 2/3 or whom it is impossible to • document the absence of CIN 2/3 prior to or as the indication • for hysterectomy should be screened until 3 documented, • consecutive, technically satisfactory negative results are • obtained within a ten year period • Women with a h/o DES exposure in utero or a h/o • cervical cancer should continue screening after • hysterectomy
Rationale • Pap Smears after hysterectomy screen the vaginal cuff • Vaginal cancer is uncommon (1 – 2/100,000 per year) • Abnormal vaginal smears are rarely of clinical significance • Women with a h/o in utero DES exposure are at increased • risk for both vaginal and cervical cancer
When to End Screening • Both Guidelines recommend against routinely screening • women after age 65 – 70 if they have received regular screening • with 3 normal results in a row • USPSTF recommends ending at 65 • ACS recommends ending at 70 • Both recommendations are arbitrary • Continue Screening for those women • Not previously screened • Those with previous screening info unavailable • Past screening unlikely • H/O cervical cancer • in utero DES exposure • Immunocompromised
Rationale • Cervical Cancer in older women is almost entirely confined to • unscreened or underscreened • Difficult to get satisfactory samples in older women • Atrophy • Cervical Stenosis • Screening associated with potential harms: • Anxiety • Discomfort • Increased costs due to false positive results
Other Recommendations • New Technologies: • New evidence-based reports (2003) show that both liquid-based and conventional cytology are acceptable screening tests. • USPSTF (2002): Evidence is insufficient to recommend for or against routinely using liquid-based cytology • ACS: As an alternative to conventional screening, liquid-based cytology may be performed every 2 years • Routine HPV Testing: • USPSTF: Evidence is insufficient to recommend for or • against HPV testing as primary screening • ACS: The technology is promising. Once the testing is • approved by the FDA, it might be appropriate • screening in addition to Pap testing for • women 30 and over. Not more frequently • than every 3 years.
Recommendations Continued • It is important to educate women—especially teens—that a pelvic • exam does not equate with a Pap test • Women who do not need a Pap test still need regular health care • visits including gynecologic care and STD screening • Current guidelines do not address usefulness of pelvic and/or • rectal exams • Referrals for patients with low-grade cervical lesions for • colposcopy may be less necessary for adolescents given the self- • limited nature of many LSIL lesions at this age group • Detection and treatment of HSIL should be the goal of adolescent • screening and referral • Insurance coverage for new technologies is not uniform—check • before ordering
Unique Scenario • You performed a routine Pap smear on a 24 yo female. The result is within normal limits with a missing endocervical component. What are the recommendations for this situation?
Unique Scenario cont… ASCCP (American Society Colposcopy and Cervical Pathology) have published recommendations stating Pap can be repeated n 1 year if this was a routine screening Pap Earlier screening at 6 months required if there was a previous abnormal Pap without 3 normal f/u Pap smears. Or patient is immunosupressed; patient has not had regular screening; a prior Pap revealed glandular abnormalities; a high risk HPV + result was obtained in the past year.
Summary • New Guidelines have changed what age to start screening and • screening intervals • New recommendations have been developed to address when • screening may be discontinued, screening of women after • hysterectomy, and the use of new technologies • Guidelines emphasize flexibility and the need to discuss • recommendations, benefits, risks, and limitations with patients • Individual patients may have different perceptions of risk and • risk tolerance which may affect their screening choices • The biggest gains in decreasing morbidity and mortality • will be by increasing screening rates among women who • have not been screened
Further Information U.S. Preventative Services Task Force Guidelines: www.ahcpr.gov/clinic/3rduspstf/cervcan/cervcanrr.htm American Cancer Society: http://caonline.amcancersoc.org/cgi/reprint/52/6/342.pdf
References • Jemal A, Murray T, Ward E, et al: Cancer statistics, 2005. CA Cancer J Clin 55:10, 2005. • U.S. Preventative Task Force: Screening for Cervical Cancer: Guide to Preventative Services. • ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists. Obstet Gynecol 102:417, 2003.