Download
1 / 21
450 likes | 4.15k Vues
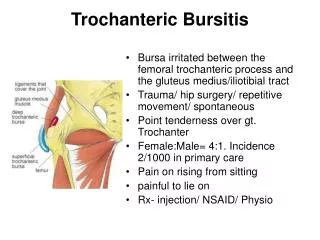
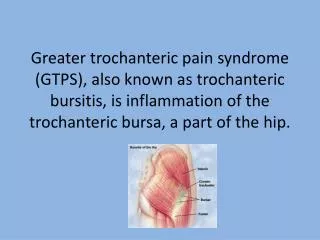
Trochanteric Bursitis. Bursa irritated between the femoral trochanteric process and the gluteus medius/iliotibial tract Trauma/ hip surgery/ repetitive movement/ spontaneous Point tenderness over gt. Trochanter Female:Male= 4:1. Incidence 2/1000 in primary care Pain on rising from sitting

E N D
Trochanteric Bursitis • Bursa irritated between the femoral trochanteric process and the gluteus medius/iliotibial tract • Trauma/ hip surgery/ repetitive movement/ spontaneous • Point tenderness over gt. Trochanter • Female:Male= 4:1. Incidence 2/1000 in primary care • Pain on rising from sitting • painful to lie on • Rx- injection/ NSAID/ Physio
The below are avoided best by core stability exercises ( physio)(1) • It is important to isolate the exact muscles for the desired effect. If the whole tummy is tensed up the stability muscles do not strengthen up well. • It is only necessary to tense the muscles up to about 25-30% of their maximum capacity to get the best effect. So trying very hard when doing these exercises is not helpful. • All the exercises are held for 10 seconds each time and done 10 times each - a total of 100 seconds. Three times a day is enough initially. • Exercise One • Lie on your front in a relaxed position. Tighten up the pelvic floor as if you are trying to stop yourself passing water, then imagine there is something hot under your tummy and try and draw it to your backbone. Do not tense up the chest or lift your hips off the surface. Once you have this, remember to keep breathing normally, not fast or particularly deep breaths.
core stability exercises ( physio)(2) • Hold for ten seconds then relax. Give yourself a short time to recover then repeat the process until you have done it ten times. You will find that when you breathe the muscles will tend to slacken, and when you tighten the muscles you’ll stop breathing. Work steadily until you can do both easily at the same time. • Exercise Two • You may need guidance from a physical therapist to do these correctly • Lie on your back with your knees bent. Gently tense up the pelvic floor again as this usually tenses up the correct muscles in the abdomen. You can add a gentle drawing down of the tummy button towards the spine. Breathe normally as before and hold for ten seconds each time. • Exercise Two - first progression. Tense up the muscles as in exercise two. Hold the muscles tense and your pelvis stable while you let one bent leg gently out to one side a short way and back. Repeat with other. Five each.
core stability exercises ( physio)(3) • Exercise Two - second progression. Hold as in the previous exercise, then lift one foot an inch off the floor only, and hold. Try and allow no movement apart from the small leg lift. Five each leg. • Exercise Two - third progression. Tense up the muscles and hold. Bend the left leg up towards the chest, reach out with the right arm and gently push against the left thigh, holding 10 seconds. Alternate for five each leg. Standing and sitting • By now you should be able to tense the correct muscles in standing and sitting and may not need to lie down to practice them anymore. You can also tense them up when doing stressful activities such as lifting a suitcase or whatever the particularly difficult movement is for you. Do them many times every day for the greatest benefit. • If you want to go to an exercise class which will help this problem, then Pilates is the best choice.
Hip Adductor Strains • groin pain is the most common finding. • quadriceps strain, adductor tendonitis are the most common • Tenderness to palpation • Rest, physio +/- NSAID
Less commonly……. Ilio-psoas bursitis and Tendonitis Iliacus Ilio-psoas • are essentially identical in terms of presentation and management. due to their close proximity.
- Bursitis • associated with hip pathology (eg, rheumatoid arthritis, osteoarthritis) • recreational injury (eg, running). • anteromedial side of the thigh to the knee pain • extension, adduction, and internal rotation of the hip pain • pain worsens slowly over weeks or months • Tenderness may occur anteriorly below the middle of the inguinal ligament and lateral to the femoral artery. • Occasionally, a palpable mass • Retroperitoneal extension (groin and pelvic complications)
Tendonitis • Acute trauma and overuse resulting from repetitive hip flexion. • insidious onset (36 months) of anterior hip or groin pain extends towards the knee • Aggravating activity with resolution soon thereafterpain all the time • Reports of an audible snap or click in the hip or groin • hip may be held in slight flexion and external rotation • shortened stride length and anterior pelvic tilt • femoral triangle and lesser trochanter tender • knees extended and subsequent elevation of the heel on the affected side. Pain (Ludloff sign) iliopsoas is the sole hip flexor activated in this position. • snapping hip sign :affected hip in a flexed, abducted, and externally rotated, then passively move the hip into extension • Treatment - Rest, physio +/- NSAID
Ischial Bursitis • See diagram • Sitting on hard surfaces/ Cycling • Palpable tender point deep in buttock • Pressure relief/ NSAID/ Physio/ Injection/ Attention to aggravating seating
Piriformis syndrome • Uncommon • Posterior hip pain – may extend to L5 and S1 neuritis sx • Worse on lifting affected leg when lying on the contralateral thigh (Pace’s test – resisted ext rotation/ abduction) • Point tenderness (lateral border of sacrum – gt trochanter • Physio/ stretches and correction of gait
Sacro-iliac dysfunction • Worse with age • Osteoarthritis, During pregnancy, some other problem which alters the normal walking pattern, inflammatory arthritides, infection (rare) • worse with standing and walking and improved when lying down. • Pain may also be present in the groin and thighs • Tender over SI ligaments • Differential: Ligament strains, A/S (rare) and infection (staph. – rare) • Rx physio, analgesics/ nsaid/ injection
OA hip • 50+ unless congenital deformity/ avasc necrosis • Stiffness as well as pain • Referral of pain to knee but no further • Tender to internally rotate first • Pain is predictor of need for intervention – esp. disturbed sleep • Differential: capsulitis as well as the above • Cycle of inflammation-cartilage loss-bony growth(osteophytes)-stiffness and pain • Family history • Rx – analgesics (pulses of NSAID), injection (specialist), resurfacing, replacement • Keep walking
Slipped Upper Femoral Epiphysis • Boys>Girls (3:1) • 10-14 years • 30% bilat • Leg held in flex/ lateral rotation • Obesity and delayed puberty • Knee pain only in some • X-ray confirms
Acetabular Labral Tear • Degenerative/ inflammatory arthritis • after twisting injury when weight-bearing/ repetitive injury. • Pain in anterior hip or groin. Stiffness locking, clicking or catching sensation in hip limited range of motion in your hip joint • Sometimes no pain symptoms Diagnosis: arthroscopy or MRI Rest, physio, analgesia and arthroscopic rx if persists more than 4/12
Stress Fracture • Femoral Neck • Up to 1.5% athletes (new recruits/ poor training) • Females –more common - osteoporosis • Deep hip pain – worse at all extremes of passive movement • Worsens progressively avascular necrosis
Referred pain from lumbar spine • Common • Quality of pain (Kelgren) – referred versus radiculitis/ radiculopathy (L5 lateral, S1 posterior, L1 and 2 anterior) • Some association with back pain • Usually, like OA, worse after sitting/ lying. Referral below knee • Usually no neurology • Examination: FROM hip, No point tenderness
Nerve Entrapment • Pain/ Paraesthesiae/ hyperaesthesia/ numbness • Anterior Obturator Nerve ( medial groin/ anterior leg with some assoc weakness of jumping on exercise : stretches and physio • Ilio-inguinal ( operations and tears of lower abdo muscles inguinal and supro-pubic sx) • Genito-femoral (sx below ing canal and on anterior aspect of hip) • Lateral Femoral Cutaneous (Meralgia Paraesthetica) • As well as physio, NSAID, local injections and anti-neuropathic meds OK
Medical Causes to bear in mind • BONE: Sacro-iliac joint instability, osteomyelitis, pelvic stress fracture, metastases • INGUINAL: Lymphadenopathy, aneurysm, hernia ( inguinal or femoral) • GENITAL:Testicular cancer, epididymitis, varicocoele • ABDOMINAL: Appendix, prostatitis, ovarian tumour
Story: • Onset – • Sudden : Muscular, labral tear, capsular strain, SUFE, • Gradual : OA, Bursitis, tendonitis • Site: • Anterior: OA, Adductor strain, Ilio-psoas(bursa and tendon), labral tear, nerve entrapment • Posterior: Sacro-iliac, Piriformis, Lumbar referal • Lateral: Nerve entrapment, OA, Trochanteric bursa, lumbar referal • Radiation • Knee : Around Hip or back • Below knee : Back (remember referred and radicul-itis/-opathy) • Sensory / Motor sx • Nerve entrapment, radicular involvement; neuralgic pain • Type of Pain • Non-mechanical (medical causes) • Mechanical – all the others Etc
Examine • Gait – watch carefully – flexed (?), all antalgic • Passive/ Active movement: flex, extend, abduct, adduct and rotate • Remember 90 degree rotation and internal rotation pain with capsulits, OA, SUFE, labral tear etc • Lateral, anterior and posterior palpation • Turn patient on side and think of the back too. • If any suspicion check the neuro. • If it doesn’t add up remember referred, entrapment, radicular and medical causes
Pain around the hip: Always be prepared to reconsider or re-examine.





![READ [PDF] Stop Hip Bursitis Pain: Greater Trochanteric, Iliopsoas and Ischial Bursitis](https://cdn7.slideserve.com/12506317/slide1-dt.jpg)