Gout and Bursitis
Gout and Bursitis. Asfand Baig. Inflammatory arthritis associated with hyperuricaemia * and intra-articular sodium urate crystals. Gout. What is the reason for the painful toe? How might you confirm the diagnosis?


Gout and Bursitis
E N D
Presentation Transcript
Gout and Bursitis Asfand Baig
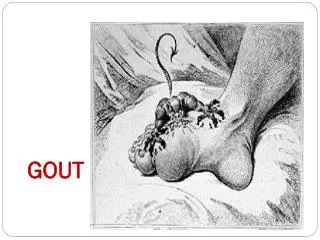
Inflammatory arthritis associated with hyperuricaemia* and intra-articular sodium urate crystals Gout
What is the reason for the painful toe? How might you confirm the diagnosis? • Acute Gout – in this case probably caused by overuse of the loop diuretic (frusemide) • Diagnosis of gout is largely clinical features (experience) • Red, swollen, extremely painful • Associated with onset of diuretic/dehydration, with some foods, males and alcohol • Site is usually first tarsel-metatarsal joint • If you need to confirm diagnosis • Uric acid: poor discriminator as lots false positives and negatives • Aspiration of synovial fluid from the joint. Look for long needle-shaped negatively birefringrnt crystals. Uric acid crystals are anisotropic, having two (birefringent) refractive indexes. James appears very unhappy. He reports to you that he has been feeling very thirsty of late due his diuretics and that three days ago the “big toe” on his right foot became extremely painful very suddenly. There was no history of trauma.Examination reveals:An acutely inflamed tarsal-metatarsal joint of the first toe on the right. The area over the joint is extremely tender to touchNo ankle swelling
Chronic hyperuricaemia • Crystals of monosodium urate monohydrate precipitation on articular cartilage, tendons of peripheral joints also in & subcutaneous tissue • Interaction between inflammatory system and urate crystals • Clinical features of acute attack due to inflammation • Attacks of gout resolve even without treatment and this is due to switching off inflammation rather than removal of crystals • Attacks can be triggered by e.g. binges of alcohol & food & stress • Some of the urate will start to deposit in joints and soft tissue – gets into synovial fluid as in blood and once there it starts to precipitate all over the structures. One it’s done that and formed crystals (it has come out of solution) the crystals trigger an inflammatory response –causes signs and symptoms 6 steps leading to Gout?
20% of patients with hyperuricaemiadevelop gout • Uric acid is the final breakdown product of purine metabolism • Production of uric acid 2/3 endogenous sources, 1/3 purine rich food • Excretion of uric acid 2/3 by kidneys, 1/3 by the bowel • Diet rich in purines – a lot of protein type foods e.g. duck. Normally recycled back into DNA – some of it doesn’t and ends up as uric acid in blood • Being fat – reduced renal clearance of uric acid – do not excrete as much, allowing it to build up in blood • Alcohol – reduced renal clearance too • Cell turnover rapid – predisposes e.g. cancer, leukaemia Who gets gout?
PAIN – spontaneous severe 75% first attack podagramonoarthritis– 1st metatarsal joint (big toe) • Swollen, red and shiny • Hot and tender • Low grade fever • recurrent attacks destroy joint cartilage and soft tissues and lead to OA: Chronic gouty arthritis Clinical features of gout
Joint aspiration (if infected synovial fluid will look pussy and yellow) • Clean not sterile • Local anaesthetic • Synovial fluid for analysis • Examined for: • Macroscopic appearance • Cell count • Gram staining • Culture (if joint infection) • Polarised microscopy (look for crystals or urate) • Performed immediately • Allow identification of urate crystals • Negatively birefringent needle shaped Investigation and diagnosis:
Differentiate between positive birefringent rhomboid shape of calcium pyrophosphate dihydrate • Chrondrocalcinosis (calcification of cartilage) often associated with haemochromatosis, primary hyperparathyroidism, also known as pseudogout(crystals of calcium being deposited in soft tissue – more square shaped, can be extremely painful and difficult to treat) Differentiate in Polarised microscopy:
NSAIDS • If contraindicated - peptic ulcer, heart failure, renal insufficiency, early post operative period • Choose intra articular corticosteroid • Systemic corticosteroid therapy may also be used e.g. prednisone 20-50mg for 7-10days • Traditional colchicine poorly tolerated & unpleasant GI upset • ICE therapy Treatment for acute gout attack
Polyarthritis • Erosions on X-ray • Tophi - deposits of urate crystals in subcutaneous areas. E.g. ears • Renal calculi (stone) Chronic gout:
Life style changes – alcohol and dietary modification, weight loss • Hypouricaemic therapy - prophylactic allopurinol (slowly) inhibits xanthine oxidase and hence uric acid production • or uricosuricsto increase clearance through kidneys • Start slowly to avoid precipitating acute attack -warn patient & cover with low dose colchicine for 6 weeks • Increase vitamin C levels as it will excrete out uric acid if marginal Treatment for chronic gout
Thiazides (e.g. bendroflumethiazide) • Act at distal convoluted tubule • Vasodilateby potassium channel activation • Prevent heart attack and stroke • Adverse effects: • Gout; low potassium & low sodium • Raised glucose & cholesterol • thiazides can be secreted into nephrons and compete for the uric acid transporter. What drug can cause gout?
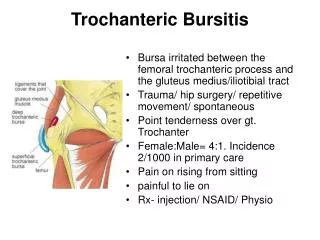
a fluid filled sac located between a bone and tendon which normally serves to reduce friction between the two moving surfaces Definition of bursae
What is the pathology of Bursitis • Acute or chronic inflammation of the bursa • What are 4 potential causes of bursitis • Chronic overuse • Trauma • Infection • Excessive pressure 15yr old male patient, Mada Hslaw, attends clinic with pain and stiffness of his right wrist. On examination the joint is swollen, warm, red and tender when pressed on. Mada sheepishly informs you that his wrist “gets alot of use”. You suspect bursitis
Avoid the precipitating activity (patient education) • Regular Icing & NSAIDS • Do not sleep/lean on affected side • Drainage & corticosteroid injection How to treat bursitis?
Inflammation (bursitis) results form repetitive use, trauma or systemic arthritis. Common areas include the shoulder, olecranon and knee (housemaid’s knee) • Shoulder subacromial, • Olecranon - student's elbow • Prepatellar • Bursitis = Housemaids knee • Infrapatella • Bursitis = Clergyman’s knee Bursitis