Download
1 / 6
60 likes | 1.02k Vues
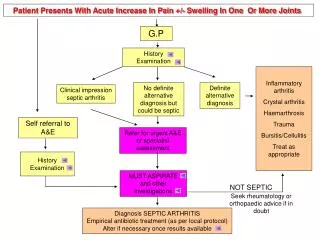
Patient Presents With Acute Increase In Pain +/- Swelling In One Or More Joints. G.P. History Examination. Inflammatory arthritis Crystal arthritis Haemarthrosis Trauma Bursitis/Cellulitis Treat as appropriate. No definite alternative diagnosis but could be septic.

E N D
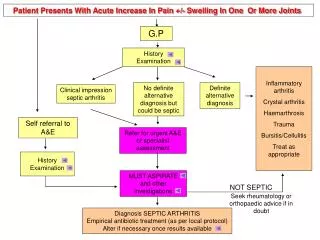
Patient Presents With Acute Increase In Pain +/- Swelling In One Or More Joints G.P History Examination Inflammatory arthritis Crystal arthritis Haemarthrosis Trauma Bursitis/Cellulitis Treat as appropriate No definite alternative diagnosis but could be septic Definite alternative diagnosis Clinical impression septic arthritis Self referral to A&E Refer for urgent A&E or specialist assessment History Examination MUST ASPIRATE and other investigations NOT SEPTIC Seek rheumatology or orthopaedic advice if in doubt Diagnosis SEPTIC ARTHRITIS Empirical antibiotic treatment (as per local protocol) Alter if necessary once results available
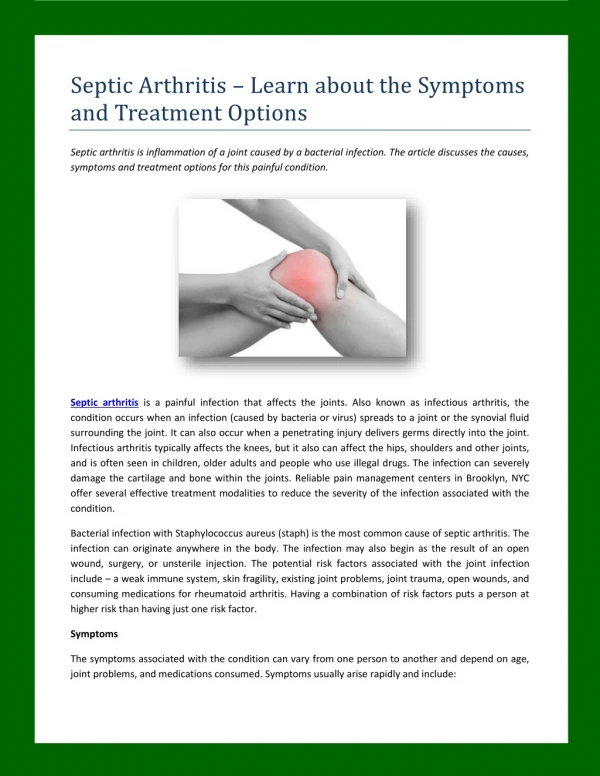
Examination • HISTORY • JointPain • JointSwelling – recent increase (symptoms often present for < 2 weeks in septic arthritis) • Note that in presence of pre-existing inflammatory joint disease the symptoms in the affected joint are out of proportion to the disease activity detected in other joints. • Systemic symptoms – e.g. fever, sweats, rigors, confusion • Factors predisposing to sepsis • - trauma, recent local infection or septicaemia, i.v. drug abuse, recent invasive procedure, pre-existing joint disease including prosthetic joints, • Drugs • Steroids and Immunosuppressants - including previous intra-articular joint injections • - could predispose to infection • Antibiotic treatment - sepsis may have been partially treated • Alternative Diagnoses • - history of psoriasis, inflammatory bowel disease or iritis would suggest seronegative spondyloarthritis • - crystal arthritis is suggested by a history of previous gout affecting the great toe • - consider haemarthrosis if there is a history of haemophilia or significant trauma • - drugs, thiazides can predispose to crystal arthropathy especially in elderly women
EXAMINATION Joint Effusion / heat / erythema / restriction of movement - if all 4 signs are present then sepsis is likely Large joints more commonly affected than small joints. The majority of joint sepsis occurs in the hip or knee 1st MTP only joint affected – consider gout. Joints involved monoarticular/polyarticular - 22% septic arthritis affects >1 joint Pyrexia May be absent in 50% of patients with septic arthritis and present in cases of crystal arthritis General Examination Look for - Signs of systemic involvement: pulse, BP - Sites of infection Skin lesions - blisters/pustules suggest gonococcal arthritis - tophi suggest gout Bursitis/cellulitis suggested by local warmth and erythema without joint effusion and without restriction of joint movement
INVESTIGATIONS • All specimens must be taken prior to antibiotic treatment • Joint Aspiration (see next section) ideally should be examined within 4 hours of aspiration • Important: The risk of missing septic arthritis in a hot joint outweighs the risk of introducing infection through needle aspiration so do not be apprehensive about performing this procedure • The only absolute contraindication to needle aspiration, outside of theatre, is a prosthetic joint • If there is overlying skin sepsis try to approach via non-infected skin • Warfarin is NOT a contraindication • Blood FBC • ESR/CRP • U&Es, LFTs • Microbiology Blood cultures x 2 (essential) • Swabs (e.g. throat, skin for C +S) • MSU • Sputum • High suspicion of TB – sputum, 3 x early morning urine • Imaging X-ray - as baseline, this is not diagnostic or urgent. It can wait until the next day • Hip aspiration may be guided by USS (seek specialist advice) • If further imaging is required an MRI as may be useful (seek specialist advice)
INVESTIGATION OF SYNOVIAL FLUID Synovial fluid must be aspirated prior to starting antibiotics, Gram stained andcultured (If affected joint is prosthetic seek orthopaedic advice) Send specimen fresh to the laboratory for immediate microscopy and culture Polarising microscopy to evaluate crystals must be carried out on all synovial fluid samples. The samples should be fresh and the microscopy performed by a microscopist experienced in crystal identification. (If unable to process samples immediately they should be stored at room temperature overnight to prevent artefactual crystal formation) Neither the absence of organisms on Gram stain, nor a negative synovial fluid culture excludes the diagnosis of septic arthritis, although they make it less likely and alternative diagnoses should be considered
Patient Group Antibiotic Choice No risk factors for atypical organisms Flucloxacillin 2g qds iv. Local policy may be to add gentamicin iv. If penicillin allergic, Clindamycin 450-600mg qds iv. or 2nd or 3rd generation cephalosporin iv. High risk of Gram –ve sepsis (elderly, frail, recurrent UTI, recent abdominal surgery) 2nd or 3rd generation cephalosporin eg cefuroxime 1.5g tds iv. Local policy may be to add flucloxacillin iv to 3rd generation cephalosporin. Discuss allergic patients with microbiology-Gram stain may influence antibiotic choice MRSA risk ( known MRSA, recent inpatient, nursing home resident, leg ulcers or catheters, or other risk factors determined locally) Vancomycin iv. plus 2nd or 3rd generation cephalosporin iv. Suspected gonococcus or meningococcus Ceftriaxone iv. or similar dependent on local policy / resistance iv drug users Discuss with microbiologist ITU patients, known colonisation of other organs (eg cystic fibrosis) Discuss with microbiologist Summary of recommendations for initial empirical antibiotic choice in suspected septic arthritis Antibiotic choice will need to be modified in the light of results of Gram stain and culture. This table is based on expert opinion, and should be reviewed locally by microbiology IV antibiotics should be used and continued for at least 2 weeks Repeat joint aspiration/surgical intervention may be required – all patients should be referred for a rheumatological or orthopaedic opinion Joints should be aspirated to dryness as often as is required Further treatment with oral antibiotics for at least 4 weeks. Do not stop antibiotics until symptoms and signs resolve, and ESR/CRP are returning to normal