Download
1 / 24
250 likes | 314 Vues
Heart disease for the lay individual

E N D
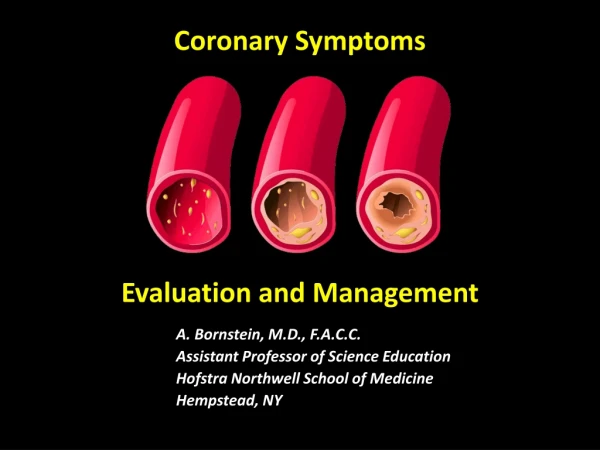
Coronary SymptomsEvaluation and Management A. Bornstein, M.D., F.A.C.C. Assistant Professor of Science Education Hofstra Northwell School of Medicine Hempstead, NY
What is Coronary Artery Disease? • As CAD develops, the arteries that supply blood to heart muscle become hardened & narrowed due to progressive buildup of cholesterol & fat forming plaque in the inner lining of the arteries, progressively obstructing blood flow. • As the plaque buildup grows, blood is able to flow through the arteries resulting in the heart muscle being unable to get adequate blood, nutrients, and oxygen it needs to continue pumping effectively especially during exercise. • This leads to chest pains due to angina pectoris &/or a heart attack (MI); most heart attacks happen when a plaque ruptures (men)or erodes (women) causing a blood clot to form that may totally block the heart muscle blood supply, causing permanent heart muscle damage (CHF) & possible dysrhythmia sudden cardiac death.
Symptoms of Coronary Artery Disease (Angina Pectoris) Cold weather, smoking and heavy meal are 3 precipitants of angina or heart attack via 3 mechanisms: • Cold causes coronary artery spasm (constricted coronary arteries), while • Cigarettes cause the blood to clot(hypercoagulable) more readily. • Redistribution of blood flow between GI tract (digestion) & heart. https://www.netterimages.com/
What is Angina; What is an MI (Heart Attack)? • Over time, CAD (repeated heart attacks or unstable angina) can also weaken the heart muscle contributing to heart failure and arrhythmias • It is difficult to estimate exactly how common heart attacks are because as many as 200,000-300,000 people in the U.S. die (~50% of all MIs) each year before medical help is sought or medical help arrives(Mortality rate: 200,000-300,000) • ~ 1 million patients visit the hospital each year with a heart attack • ~ 1out of 5 deaths (20%) are due to a heart attack
Heart Attack (MI) Due to Plaque Rupture Triggering Acute Thrombus Formation
Scope of the Problem: United States ER Visits 141.4 million patient annual ER visits in 2014 (18% from 2006) making chest pain 2nd most common complaint Of these, 6,315,000 ER chest pain visits Of these, 1,633,000 admitted for angina/MI 60% elderly (age > 65); 46% women 66% UA/NSTEMI (partial MI); 33% STEMI (total MI); The average patient 11,000 diagnoses of MI were missed & patient sent home; 77% UA/NSTEMI (partial MI); 23% STEMI (total MI) Former VP Dick Cheney CVD will be #1 cause of death worldwide by 2020 Moore BJ (IBM Watson Health), Stocks C (AHRQ), Owens PL (AHRQ). Trends in Emergency Department Visits, 2006–2014. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb227-Emergency-Department-VisitTrends
Not Chest Pain Symptoms Indicative of Serious Pathology Momentary chest discomfort, often characterized as fleeting or electrical shock. Chest discomfort or pain is with an MI is unrelenting, typically lasting for several minutes to hours. Momentary chest discomfort is more likely to result from musculoskeletal injury or inflammation (costochondritis), nerve pain (e.g., rib fracture, strained muscle in the chest wall, or shingles involving the chest). Pinpoint chest discomfort or CP that worsens with positional changes, breathing, or touching the area. Heart pain is usually diffuse &/or radiating. Discomfort that changes with breathing is more likely to involve the lungs (e.g., pleurisy, inflammation of the lung membranes, pneumonia, or asthma). Chest discomfort that gets better with exercise. Heart-related pain typically worsens with exercise. Sharp chest pain that improves with movement is more likely to have other causes. AHA Heart Disease and Stroke Statistics 2004 Update, and Mosca et al., Circulation 2007; 115: 1481-1501.
CAD & Heart Attack Risk Factors • Bad genes (hereditary factors, family history) • Age • Being male (MI at an earlier age) • Menopause in females • High blood pressure • Smoking • Obesity (Metabolic syndrome) • Diabetes mellitus • Low levels of physical activity • Too much unhealthy fat in the diet • LDL (‘bad’) cholesterol & HDL (‘good’) cholesterol • Homocysteine, CRP, &/or fibrinogen (markers of inflammation & increased clotting tendency)
Calculating Cardiovascular Mortality Risk • Computer calculator algorithms have been developed for assessment of cardiovascular risk in people with different lifestyles &ages,most accurate if cholesterol levels & blood pressure levels are also provided. The calculator then provides an estimate of a person’s “heart age” & controversially, predicts when he/she will probably suffer a heart attack or stroke, & % chance of a heart attack or stroke over the next decade.Patients understanding their heart age can be a real wake up call for people at risk & that all-important nudge to make lifestyle changes to improve heart health. • It means a woman of 41, with an unhealthy lifestyle, medical problems such as diabetes, and a family history of heart disease could be warned that she is highly likely to suffer a heart attack or stroke by the age of 51. Another woman the same age, with a healthy lifestyle and no family history could be told she is likely to get to the age of 83 before being consigned to such a fate. • A man of 50 who smokes, suffers from a number of medical problems, and a family history of heart disease, could be told he is likely to have a heart attack or stroke by 56. • A healthier man of the same age, with no family history could expect to live to 79 without a heart attack or stroke, according to the calculator. http://www.cvriskcalculator.com/ TRY IT YOURSELF!!
Calculating Cardiovascular Mortality Risk http://www.cvriskcalculator.com/ http://static.heart.org/riskcalc/app/index.html#!/baseline-risk
Mortality Rates in Women 6500 4500 2500 1600 1200 800 400 0 At every age, more women die from heart disease than from cancer Coronary artery disease Stroke Lung cancer Breast cancer Colon cancer Endometrial cancer Mortality Rate per 100,000 50% of women (1 in 2) will die from CVD compared with 4% (1 in 25) who will die from breast cancer 45–49 50–54 55–59 60–64 65–69 70–74 75–79 80–84 85+ Age (years) National Center for Health Statistics. 1999:164-167.
Cardiovascular Disease in Women • 38.2 million women (34%) are living with cardiovascular disease and a much larger population is at significant risk. • Heart disease and stroke are the #1 and #2 killers of women over age 25. • 1 in 30 die of breast cancer, but 1 in 3 die of cardiovascular disease or stroke. • 66,000 more women than men die/year of cardiovascular disease; this represents 54% of deaths in women compared to 46% of deaths in men. AHA Heart Disease and Stroke Statistics 2004 Update, and Mosca et al., Circulation 2007; 115: 1481-1501.
Cardiovascular Symptoms in Men vs. Women AHA Heart Disease and Stroke Statistics 2004 Update, and Mosca et al., Circulation 2007; 115: 1481-1501.
Women Have Smaller Coronary Arteries After correcting for (BSA) body surface area, women’s arteries are smaller in diameter This can seriously affect symptoms from anything that reduces diameter: Stenosis Endothelial dysfunction Smaller arteries Endothelial dysfunction Adapted from Bellasi et al, New insights into ischemic heart disease in women. Cleveland Clinic journal of medicine; 74: 585-594
Gender Differences in Atherosclerosis Women suffer more plaque erosion (left) compared to plaque rupture in men (right), leading to more acute coronary syndromes (unstable angina & incomplete MI in women), making diagnosis more difficult and leading to delays in treatment. Plaque rupture in men Plaque erosion in women NEJM 1999
NIH-NHLBI-Sponsored WISE Study Women’s Ischemia Syndrome Evaluation • Persistent chest pain with no evident obstructive disease is nota benign condition. • Those with persistent chest pain had 2X the number of CV events (MIs, strokes, CHF & CV deaths) compared to those without persistent chest pain. • ~ 50% of women who are sent home with “normal coronaries” ??? continue to experience disabling symptoms and chest pain. • 673/936 (72%) of women enrolled in WISE had persistent chest pain. • Possibly caused by coronary microvascular disease &/or macrovascular endothelial dysfunction. Johnson D, et al Eur Heart Journal 2006
Menopause and Risk of Coronary Heart Disease Annual Occurence of Heart Attack/1000 Age (in years) “Menopausal status as a risk for coronary artery disease” Arch Intern Med 1995;155:57-61
Women’s Early Warning Signs of a Heart Attack Weeks before heart attack Unusual fatigue (70.7%) Sleep disturbance (47.8%) Shortness of breath (42.1%) Indigestion (39.4%) Chest pain (29.7%) Immediately at time of heart attack Shortness of breath (57.9%) Weakness (54.8%) Fatigue (42.9%) Chest pain (57%) McSweeney, JC et al. Circulation 2003; 2619-2623
Causes of Chest Pain Other Than Atherosclerotic Cardiac Disease (ASCVD) Chest Pain: Gastrointestinal Problems • GE reflux disease (GERD) • Esophageal contraction disorders • Esophageal hypersensitivity • Esophageal rupture or perforation • Peptic ulcers • Hiatal hernia • Pancreatitis • Gallbladder problems Chest Pain: Bone, Muscle, or Nerve Problems • Rib problems • Muscle strain • Shingles Chest Pain: Cardiac (not ASCVD) • Myocarditis • Pericarditis • Hypertrophic cardiomyopathy (HOCM) • Mitral valve prolapse • Coronary artery dissection Chest Pain: Lung (Pulmonary) Problems • Pleuritis • Pneumonia • Pulmonary embolism • Pneumothorax • Pulmonary hypertension • Asthma Chest Pain: Nonspecific • Panic attacks
Harvard Nurses’ Health Study: BMI & Relative Risk of CHD Over 14 Years • Normal weight: BMI is 18.5-24.9 Overweight: BMI is 25-29.9 Obese: BMI is >30 • Relative risk of CHD increases for BMI >23; diabetes mellitus risk increases for BMI >22 • Risk also increases significantly for weight gain of 5 kgms or more after age 18 years Dietary Fat Intake and Risk of Coronary Heart Disease in Women: 20 Years of Follow-up of the Nurses' Health Study Kyungwon Oh Frank B. Hu JoAnn E. Manson Meir J. Stampfer Walter C. Willett American Journal of Epidemiology, Volume 161, Issue 7, 1 April 2005, Pages 672–679,https://doi.org/10.1093/aje/kwi085
Diabetes as a CHD Risk Equivalent • 10-year risk for CHD 20% • High mortality with established CHD • Higher mortality with acute MI • Higher mortality post acute MI Prevalence of diabetes has increased over 25% in past 15 years in California, paralleling 50% increase in overweight/obesity