Download
1 / 1
20 likes | 154 Vues
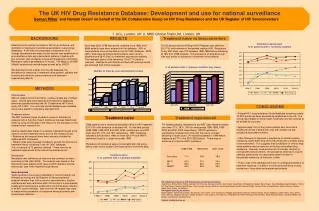
Number of tests by year and treatment status. Treatment experienced. Treatment naïve. RESULTS. Treatment naïve vs Seroconverters. % of patients with 1 primary mutation (any class). CONCLUSIONS. BACKGROUND. METHODS. 20. 18. 16. 14. 12. 10. 8. 6. 4. 2. 0. 1996-1998.

E N D
Number of tests by year and treatment status Treatment experienced Treatment naïve RESULTS Treatment naïve vs Seroconverters % of patients with 1 primary mutation (any class) CONCLUSIONS BACKGROUND METHODS 20 18 16 14 12 10 8 6 4 2 0 1996-1998 1999-2000 2001-2003 Naive Seroconverters The UK HIV Drug Resistance Database: Development and use for national surveillance Deenan Pillay1 and Hannah Green2 on behalf of the UK Collaborative Group on HIV Drug Resistance and the UK Register of HIV Seroconverters 1. UCL, London, UK 2. MRC Clinical Trials Unit, London, UK Determining the clinical correlates of HIV drug resistance, and estimation of resistance surveillance parameters, require large databases. A UK-wide non-proprietary collaboration of all virology laboratories and major clinical centres was established to pool resistance data and interpretation patterns, together with pre- and post- test virological, clinical and therapeutic information. Resistance data is generated by “in house”, VGI (Bayer), and ABI (Abbott) sequencing methodologies as well as by VIRCO. We describe the first outputs from the UK database; the prevalence of resistance in treatment naïve patients, patients with acute/recent infections (seroconverters) and treatment experienced patients. Treatment experienced: % of patients with 1 primary mutation As of May 2003, 9798 test results, obtained since 1996, from 6684 patients have been entered into the database. 60% of these patients have clinical data in the UK CHIC database. 2279 (23%) tests were performed whilst patients were naive to treatment and 5815 (59%) on treatment experienced patients. The treatment status of the remaining 1704 (17%) tests is unknown. Resistance test failures and tests with missing results are excluded from further analyses. Of 152 seroconverters fulfilling the UK Register case definition, 26 (17%) had evidence of transmitted resistant HIV. Resistance to any ART class was 15% between 1996-1998 before stabilising at 18% from 1999 onwards. The prevalence of resistance over time was similar to resistance in treatment naïve patients. • Clinical data • Without related clinical information, resistance data are of limited value. Clinical data were obtained from electronic databases wherever possible including the UK Collaborative HIV Cohort study (UK CHIC). If no accurate clinical database was available, clinics were asked to complete a standard form. • Treatment status • The ART treatment status of patients (naïve to treatment or experienced) at the time of each resistance test was determined either by using clinical data or the reason for the test given on the resistance test request form. • Various checks were made on a sample of patients thought to be naïve to confirm treatment history prior to the resistance test: • Resistance test request forms were manually checked for additional ART information • Patient notes were manually checked to assess the accuracy of treatment history contained in the UK CHIC database. • Out of a sample of 72 patients checked, 7 were found to be treatment experienced at the time of the resistance test. • Resistance • Resistance was defined as at least one key (primary) mutation according to IAS-USA (2003). The analysis was based on the first test for each patient whilst naïve to ART treatment and the first test per year when treatment experienced. • Seroconverters • Tests reported to have been undertaken in ‘seroconverters’ are followed up through the UK Register of Seroconverters to establish whether they fulfil a common case definition; that the resistance test was performed within 18 months of a documented negative HIV antibody test or laboratory confirmed acute infection in an ART-naïve individual. Data from the UK register was used to measure the prevalence of resistance amongst patients with acute/recent infections. • A large HIV-1 drug resistance clinical database containing nearly 10,000 results has been successfully established in the UK. The clinical data related to these results have been and will continue to be audited for accuracy. • Approximately 15% of drug naïve patients who have had a resistance test are infected with virus with at least one key resistance associated mutation. • Little difference is observed in prevalence of resistance when comparing nearly 2000 drug naïve individuals with a smaller group of seroconverters. This suggests that surveillance of chronic drug naïve patients may be useful for monitoring transmitted drug resistance. However, because they are chronically infected (in contrast with seroconverters), the prevalence observed in a given calendar period does not necessarily reflect the level of transmitted resistance at that point in time. • Future uses of the database will focus on virological predictors of treatment response, in addition to continual surveillance of drug resistance in drug naïve and experienced patients. 1966 patients had a resistance test whilst naïve to ART treatment; 270 (14%) with evidence of resistant HIV. For the time periods 1996-1998, 1999-2000 and 2001-2003, resistance to any ART class was 9%, 15% and 16% respectively. NRTI resistance followed a similar trend. After an initial rise in PI and NNRTI resistance, there is no clear trend after 1999. Prevalence of resistance was not associated with risk group, ethnic origin or the closest CD4 measurement to the test date. For treated patients, resistance to any ART class remained stable over time (71%, 78 %, 78% for time periods 1996-1998, 1999-2000 and 2001-2003 respectively). NNRTI resistance significantly increased over time with the rate of increase declining in recent years. PI resistance peaked in 1999 before stabilising at 27% in the 2001-2003 period. There was no evidence of a trend in NRTI resistance. Treatment naive: % of patients with 1 primary mutation UK Collaborative Group on HIV Drug Resistance Steering Committee: Judy Breuer, Sheila Burns, Sheila Cameron, Ian Chrystie, Duncan Churchill, John Clarke, David Dunn, Philippa Easterbrook, Barry Evans, David Goldberg, Mark Gompels, Teresa Hill, Paul Kellam, Andrew Leigh-Brown, Clive Loveday, Ryanne Matthias, Anna Maria Murdin-Geretti, Andrew Phillips, Deenan Pillay, Kholoud Porter, Anton Pozniak, Caroline Sabin, Peter Tilston, Ian Williams UK Register Steering Committee: Abdel Babiker, Valerie Beral (Chair), Ray Brettle, Chris Carne, Janet Darbyshire, Philippa Easterbrook, Noël Gill, Richard Gilson, David Goldberg, David Hawkins, Don Jeffries, Anne Johnson, Margaret Johnson, George Kinghorn, Linda Lazarus, Ken McLean, Philip Mortimer, Andrew Phillips, Deenan Pillay, Sarah Rowland-Jones, Jonathan Weber, Ed Wilkins; Coordinator: Kholoud Porter Contact: d.pillay@ucl.ac.uk