Acute Transfusion Reactions
390 likes | 1.44k Vues
Acute Transfusion Reactions. Clinical Symptoms and Laboratory Investigation. Acute Allergic Febrile Hemolytic Anaphylactic Bacterial Contamination (Sepsis) Circulatory Overload Transfusion Related Acute Lung Injury (TRALI). Delayed Alloimmunization Hemolytic Transmissible Diseases

Acute Transfusion Reactions
E N D
Presentation Transcript
Acute Transfusion Reactions Clinical Symptoms and Laboratory Investigation
Acute Allergic Febrile Hemolytic Anaphylactic Bacterial Contamination (Sepsis) Circulatory Overload Transfusion Related Acute Lung Injury (TRALI) Delayed Alloimmunization Hemolytic Transmissible Diseases Graft vs Host Disease Iron Overload Post Transfusion Purpura Types of Transfusion Reactions
Definition • Acute Transfusion Reaction: • Reactions occurring at any time up to 24 hours following a transfusion of blood or components.
The Most Common Cause of Acute Immediate Intravascular Hemolysis • Failure to identify the patient with the donor unit at the time of administration • Collecting pre-transfusion specimen from the wrong patient • Incorrectly labelled specimens • Unlabelled specimens that are labelled after leaving the bedside (in the lab or at the nursing station)
Administration Guidelines (Preparation) • Have physician obtain informed consent and document the indications for the transfusion in the chart • Assess the patient’s understanding of the procedure • Describe the procedure, component, length of transfusion and expected outcome to the patient • Instruct patient to report ANY unusual symptoms immediately
Administration Guidelines (con’t) • Obtain and record baseline vital signs • Assess for any pre-transfusion symptoms which could be confused with a transfusion reaction • Premedicate patient with prophylactic medication as per physician’s orders • Use appropriate equipment • Obtain the component from the lab
Administration Guidelines (con’t) • Inspect the component for leaks, abnormal cloudiness, color, clots, excessive air. Check that the component is not expired. Mix well • Check the physicians order for transfusion. Ensure component type is correct. • Do not underestimate the importance of patient and product identification that MUST occur at the bedside • If the patient is not wearing a ID bracelet DO NOT proceed • Contact the lab if there are ANY discrepancies
Administration Guidelines (con’t) • Start the infusion slowly (5 mL/minute or less for first 15 minutes) • Symptoms of a severe transfusion reaction are usually manifested during the first 50 mL or less of blood infusion • If possible, remain with the patient the first 10-15 minutes of the transfusion • Document the identifying individuals, date and time transfusion initiated in the chart • The chart must also contain the unit identifying number, ABO/Rh • Keep all identification attached to the blood container until the transfusion is completed
Administration Guidelines (con’t) • Before leaving the bedside, remind the patient to notify you immediately if they feel anything unusual • Monitor and record vital signs as defined in nursing policy • At the end of the transfusion, record end times, volume transfused and immediate response (i.e. no reaction noted, reaction noted…)
GENERAL Fever Chills Muscle ache,pain Back pain Chest pain Headache Heat at the site of infusion or along vein Nervous System Apprehension, impending sense of doom Tingling, numbness Respiratory Tachypnea Apnea Dyspnea Cough wheezing Signs & Symptoms
Gastrointestinal Nausea Vomiting Pain, abdominal cramping Diarrhea (may be bloody) Renal Changes in urine volume Changes in urine color Cardiovascular Heart rate Blood Pressure Circulatory Bleeding Cutaneous Rashes, Hives(urticaria) Itching Signs & Symptoms
Signs in an Unconscious Patient • Weak Pulse • Fever • Hypotension • Visible hemoglobinuria • Increased operative bleeding • Vasomotor instability • Tachycardia, brachycardia, hypotension • Oliguria/anuria
Remember Reactions from different causes can exhibit similar manifestations; therefore, every symptom should be considered potentially serious and transfusion should be discontinued until the cause is determined
Immediate Actions to Take • Stop the Transfusion • Notify the attending physician and the laboratory immediately • Do clerical check at bedside of identifying tags and numbers • If symptoms are urticaria and pruritis only, consider administering antihistimine • If symptoms disappear continue transfusion • If additional symptoms or hives and itching do not disappear discontinue transfusion • Collect blood specimen and first voided urine
Immediate Actions to Take • Treat patient symptoms • as per physician instructions • Take vitals • Pulse • Temperature • Blood Pressure • Document thoroughly • Complete reaction form • Send form, bag, tubing and set to laboratory
Laboratory Actions when Notified of Suspected Reaction • Quarantine all other crossmatched units • When Reaction form, unit, set, tubing, urine received • Centrifuge specimen • Clerical Check • Review Symptoms • To determine extent of investigation required
Clerical Check • Check test results vs. interpretation • Check tag information with bag information (unit number, ABO/Rh) • Check Pre-transfusion specimen information with tag information (name, number) • Check that information on pre-transfusion specimen is identical to post-transfusion
Visual Inspection • Compare plasma color of pre-transfusion and post-transfusion specimens • Is post-transfusion specimen hemolyzed? • If yes, ensure that hemolysis is not due to difficult collection (recollect if necessary) • If still yes, notify physician immediately • Check contents of unit for hemolysis • Check blood in tubing for hemolysis
Direct Antiglobulin Test (DAT) • To determine if there is in vivo sensitization • May be negative if intravascular hemolysis has occurred • If positive, perform monospecific DAT to determine if it is IgG, C3 or both
Extended Testing • ABO/Rh on pre and post transfusion specimens • ABO/Rh on donor unit • Antibody screen on pre and post transfusion specimens • Antibody Investigation, positive • DAT on pre transfusion specimen and donor unit
Reporting • Classified as to type of reaction given symptoms and investigation outcome • Should be signed off by laboratory physician or designate • Reference for follow up for any attending physician questions regarding future transfusions given the patient’s clinical need • Patient should be informed of reaction and outcome
Reporting • Should include future pre medication or special requirements, if applicable • Examples • Antihistamines • Anti pyretics • Washed blood (when anaphylactic reactions are under investigation and results are not back yet) • Antigen negative blood if a clinically significant antibody is identified
Reporting • Hospitals should report all severe and fatal reactions to the blood supplier • Health Canada requires that CBS Head Office advise them within 24 hours of a fatal reactions and as soon as possible (within 15 calendar days), of a life-threatening or permanently disabling reaction. To comply with this requirement, hospitals should report these types of adverse reactions immediately to their local CBS.
Future Transfusions • Patient should be notified if special requirements are necessary • Antibody card • Transfusion reaction investigations and reports should be retained indefinitely by the laboratory
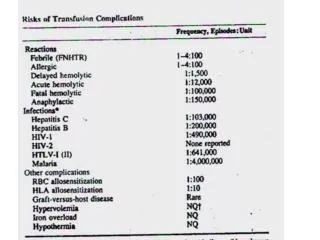
Risk of Suffering a Transfusion Reaction • RBC Alloimmunization: 1-2% • Febrile Non-Hemolytic • to Platelets: 20-30% • to RBC: 1% • Allergic (mild): 1-3% • Circulatory Overload: 1% • Acute Hemolytic: 1:12,500 • Fatal: 1/600,000 • Anaphylaxis: 1/25, 000
The Message • The risk of a severe transfusion reaction is low but health care professionals must have documented procedures for recognition and identification of the adverse effects of transfusion • The outcome • Better informed patients, nurses, physicians and laboratory personnel resulting in quality patient care