Transfusion Reactions
Transfusion Reactions. Introduction. Blood transfusion is safe, effective way to correct hematology defects and crucial part of supportive care of some patients Sometimes unwanted results may occur during or after transfusion One of these is transfusion reactions. Transfusion Reactions.


Transfusion Reactions
E N D
Presentation Transcript
Introduction Blood transfusion is safe, effective way to correct hematology defects and crucial part of supportive care of some patients Sometimes unwanted results may occur during or after transfusion One of these is transfusion reactions
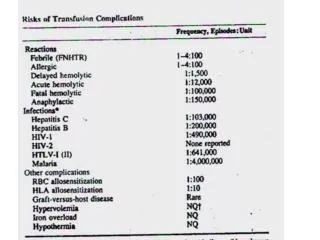
Transfusion Reactions • They are adverse reactions associated with the transfusion of blood and its components • 3% of individuals receiving blood transfusions have a transfusion reaction
Transfusion reactions • Non-threatening to fatal (Fatal ~ 1/50000) • Immunological or Non-immunological • May or may not cause RBC destruction • Immediate to delayed • Immediate – rapid onset (<24 hours) • Delayed – >24 Hours,Occur days, weeks, • May involve infectious agents
Transfusion Reactions • Most common causes of transfusion related DEATHS: • Improper specimen identification • Improper patient identification • Antibody identification error • Crossmatch procedure error • Most transfusion reactions (not all) are the result of human error.
Immediate Hemolytic Reactions • Most common cause is ABO incompatibility (clerical error) • Red cell destruction due to complement activation by IgM • RBCs hemolysed due to reaction between Abs in recipient (A & B) & Ags on donor’s RBCs • As little as 10-15 mL can trigger a reaction
Symptoms • Fever • Pain at infusion site • Back/chest pain • Physical signs • Fever • Hypotension • Bleeding • Renal failure • Hemoglobinuria
Steps taken if hemolytic reaction is suspected • Stop transfusion • Keep IV line open with physiologic saline • Perform bedside clerical checks • Contacts patient’s physician & blood bank • Return unit, set & attached solutions to Lab • Collect suitable blood samples for evaluation • Microbiological on unit, culture of patient’s blood, Check for DIC, Renal function
Treatment • Treat hypotension by fluid replacement • Maintenance of renal blood flow • Replacement of depleted coagulation factors • Dialysis in case of renal failure
Transfusion of RBCs Allo-Abs • Rarely, patient’s red cells can be hemolyzed by Abs in transfused whole blood or plasma • Caused by anti-A or Anti-B in certain plasma products • Cryoprecipitate • Factor VIII or IX • Positive DAT, Anti-A or Anti-B can be eluted from red cells
Transfusion Induced Alloimmunization • Ags are administered during transfusion • In 1st transfusion Induce alloantibodies • This will cause problems in subsequent transfusions • Prior transfusion beneficial in some cases • E.g. renal transplantation is more successful in patients with prior multiple transfusions
Pseudo-Hemolytic Reactions • Some transfusions may appear to be immediate HTR, but they are not due to immune RBC destruction • These are called pseudo-hemolytic TR
Delayed Hemolytic Transfusion Reactions • DHTRs occur at least 24 hrs after transfusion • Mediated by IgG antibodies • Patient previously exposed to RBC antigen and has low antibody titer until exposed again • Cannot be detected in crossmatch • Rh, Kidd, Duffy, and Kell
Delayed Hemolytic Transfusion Reactions • Patients have no symptoms • The only indication is a fall in hemoglobin • Diagnosis made by re-crossmatch • DAT is usually positive • Elutions are performed to identify Ab
White Cell ReactionsFebrile Reactions • Most common, 2% of all transfusions • Caused from HLAs on the WBCs of the donor that react with the recipient antibody • Any component that contains WBCs could cause FNHTRs • Cytokines IL-1, 6,8 and Tnf-alpha generated in stored blood/products. • Determining factor is age of blood products • Leukocytes reduced units may be given
Pulmonary Infiltrates • Transfusion Related Acute Lung Injury • Can be due to: • Hypervolemia • Donor antibodies that react with the recipient’s granulocytes or vice versa • which cause embolism to blood vessels in lung tissue • Then fluids and proteins leak into alveolar space/ interstitium • The lungs fill with a high-protein fluid • Patient displays acute respiratory insufficiency with x-ray showing pulmonary edema without cardiac failure
Graft-versus-Host Disease • Rare but fatal condition that has a 90% mortality rate • May be caused by donor lymphocytes transfused into an immunocompromised recipient • acute graft-versus-host-disease is characterized by selective damage to the liver, skin and mucosa, and the gastrointestinal tract • Any components that contain T-lymphocytes should be irradiated to prevent GVHD
Platelet ReactionsPost Transfusion Purpura (PTP) • PTP characterized by severe consumptive thrombocytopenia • Typically in women with a history of pregnancy, immunized with Human platelet Specific Alloantigen (HPA) • Thrombocytopenia is self-limiting and lasts for 2-6 weeks • Occur in patients who are negative for HPA-1a
Plasma Protein ReactionsAnaphylaxis • Cause • Infusion of IgA proteins into Pt with IgA antibodies • IgA deficiency about 1 in 700 • Hypotension and bronchospasm • Transfusion should be stopped immediately • IgA deficient patients should be transfused with blood products lacking IgA
Urticaria • Second most comon type of TR • Characterized by a pruritic rash during or following transfusion • Allergic reactions are IgE mediated. • These reactions are usually attributed to hypersensitivity to soluble allergens found in the transfused blood component. • Associated with anti-IgA in recipients who are IgA deficient.
Urticaria • If not accompanied by other signs or symptoms, transfusion can be continued • Anti-histamines are given
Massive Blood Transfusion • Massive transfusion, defined as the replacement by transfusion of more than 50 percent of a patient's blood volume in 12 to 24 hour, • may be associated with a number of hemostatic and metabolic complications
Bleeding due to Dilution of clotting factors • Patients receiving large volumes of blood can develop a bleeding disorder due to dilution of coagulation factors & platelets • Stored blood has low levels of the: • clotting factors VIII and V • Does not contain functional platelets • Significant depletion occur when patient’s blood is replaced more than twice within 24 hrs
The administration of: • platelet concentrates • cryoprecipitate • and fresh frozen plasma • can prevent this complication to patients receiving massive transfusions
Citrate Toxicity & Hypocalcemia • Large amounts of citrate are given with massive blood transfusion • Since blood is anticoagulated with sodium citrate. • A decline in the plasma free calcium concentration is the potential complication of citrate infusion and accumulation. • Calcium supplements should be given if patient has evidence of hypocalcemia • This rarely occur unless one unit is given every 5 minutes or a patient has impaired liver function
Hypothermia • Rapid transfusion of multiple units of chilled blood may reduce the core temperature abruptly • This can lead to cardiac arrhythmias. • Thus, during massive transfusion, a commercial blood warmer should be used to warm blood toward body temperature during infusion.
2,3 DPG Deficiency • During storage erythrocytes concentration of 2,3-DPG falls • This increases affinity of Hb to O2 → less efficient in delivery of O2 • Rapid infusion of 2,3-DPG depleted cells could contribute to tissue hypoxia • Also, the use of CPD-A avoid this problem as rate of depletion decreases gradually
Hyperkalemia • Plasma potassium levels in stored blood increase due to passive leakage of potassium out of red cells • By 3 weeks the level is approx. 30 mEq/l • This excess potassium does not usually lead to a significant rise in the plasma potassium concentration due to movement into the cells, urinary excretion, and dilution. • However, infants and patients with renal impairment may develop hyperkalemia.
Microemboli • During storage, white cell & platelet fragments aggregate to form microscopic debris or microemboli • These can pass through standard blood bank filters • They can embolize to the lungs, but have not been reported to cause morbidity