Download
1 / 23
230 likes | 334 Vues
William G. Ward, Matthew T. Cline, Fred J. Dorey* Wake Forest University Health Sciences, Winston-Salem, NC, *Department of Pediatrics, USC Keck School of Medicine, Los Angeles, CA. Factors Influencing Sarcoma Referral and Treatment. What Is An Unplanned Resection?. Lack of …

E N D
William G. Ward, Matthew T. Cline, Fred J. Dorey*Wake Forest University Health Sciences, Winston-Salem, NC, *Department of Pediatrics, USC Keck School of Medicine, Los Angeles, CA Factors Influencing Sarcoma Referral and Treatment
What Is An Unplanned Resection? • Lack of … • Preoperative imaging modalities • True wide resection
Unplanned Resections • Difficult reresection for oncologic surgeon • Increased morbidity for sarcoma patients • Reresection • Additional hospital stay • Higher rate of local recurrence
Primary Question What factors influence treatment prior to referral? • Insurance status • Race • Age • Tumor size • Bone vs. Soft-tissue
Hypothesis • Patients with insurance would be more likely to have undergone an unplanned resection prior to referral
Demographic Information • 401 Sarcoma Patients • 172 Bone and 229 Soft Tissue Sarcomas • 183 Females, 218 Males • Average age 48 (1 to 95) Results • Local recurrence-free survivorship = 91.9% ± 1.65% • Overall survivorship = 67% ± 2.4% at 5 years.
Sarcoma Number Osteosarcoma 74 Malignant Fibrous Histiocytoma 56 Liposarcoma 52 Chondrosarcoma 41 Myxofibrosarcoma 31 Synovial cell Sarcoma 24 Ewing's Sarcoma 22 Other 20 Leiomyosarcoma 17 Malignant Peripheral Nerve Sheath Tumor 14 Pleomorphic Sarcoma 14 Sarcoma (unspecified) 14 Fibrosarcoma 12 Rhabdomyosarcoma 6 Epithelioid Sarcoma 4 Diagnostic Information
Insurance Status and Unplanned Resection • Patients on Medicaid were less likely have an unplanned resection (p=0.14)
Race and Unplanned Resection • African Americans were less likely to have an unplanned resection (p=0.05) • African Americans were not more likely to be uninsured or on Medicaid
Age and Unplanned Resection • Patients under the age of 18 were less likely to have an unplanned resection. (p=0.004)
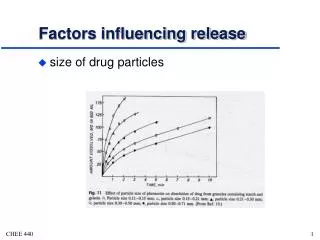
Tumor Size and Unplanned Resection • Patients with tumors 5cm at initial resection were more likely to have an unplanned resection (p < 0.001)
Unplanned Resections Based on Tumor Size p < 0.001
Soft Tissue or Bone Tumor and Unplanned Resection • Patient with bone tumors were less likely to have an unplanned resection (p < 0.01)
Logistic Regression Analysis of Local Recurrence Following Reresection Odds ratio = 3.027* *Multi-variant analysis taking into account tumor size. Dependent variable = local recurrenceIndependent variable = plan vs unplanned resection
Discussion • Our impression is that most unplanned resection were performed in situations where the diagnosis of malignancy was not included in the differential diagnosis. • Evidence…unplanned resections less likely to occur with larger tumors, patients under the age of 18, and bone tumors.
Teaching Point • Whenever treating a “suspicious” mass always include malignancy in the differential diagnosis. • Avoid unplanned resections – consider early referral to oncologic surgeon and/or appropriate preoperative imaging. • Consider preoperative biopsy • FNA/aspiration • Transilluminate all suspected ganglions
Conclusion - Summary • Those less likely to undergo an unplanned resection... • Patients with larger lesions, p<0.001 • Patients under the age of 18, p=0.004 • Patients with bone tumors, p<0.01 • African Americans, p=0.05 • Patients on Medicaid, p=0.14 • Patients subjected to unplanned resections are three times more likely to have a local recurrence following definitive re-resection.