Cleft Anomalies
Cleft Anomalies. Sharon Joo , PGY 1 UNSOM-Pediatrics Nursery. Epidemiology. CPA is more common in females CLP is more common in males Differences in ethnic groups: Native Americans (1 in 230 to 1,000) Asians (1 in 400 to 850) Caucasian population (1 in 2,500)

Cleft Anomalies
E N D
Presentation Transcript
Cleft Anomalies Sharon Joo, PGY 1 UNSOM-Pediatrics Nursery
Epidemiology • CPA is more common in females • CLP is more common in males • Differences in ethnic groups: • Native Americans (1 in 230 to 1,000) • Asians (1 in 400 to 850) • Caucasian population (1 in 2,500) • Least common in African Americans (1 in 1,300 to 5,000)
Cleft Palate • 4 variants of cleft palate: • Nonsyndromic cleft lip with cleft palate • Nonsyndromic cleft palate • Syndromic cleft lip with cleft palate • Syndromic cleft palate • Anatomical boundaries: • Primary Palate • Secondary Palate Normal: closure from alveolar ridge anteriorly to the uvula
Variants of Cleft Palate Current Diagnosis: Orofacial Clefting
Emedicine: http://emedicine.medscape.com/article/995535-overview#showall
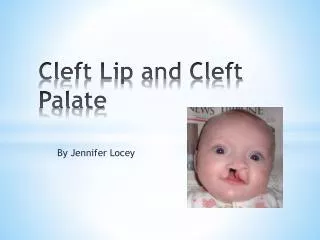
Cleft Lip Current Diagnosis: Orofacial Clefting • 4 variants of Cleft Lip • Complete • Incomplete • Bilateral • Unilateral
Incidence • Recurrence risk • for the family of a child who has isolated CLP is about 4% • the family of a child who has isolated CPA is about 2% • Increased risk of clefting if >1 child born with clefting, parent affected or depending on severity of clefting • Occurrence rate: • Cleft lip and palate: 50% • Cleft palate only: 30% • Cleft lip only: 20% • Unilateral cleft lip and bilateral cleft lip: 9:1
Embryology • Clefting defects occurs between the 6th- 9th weeks of gestation • Primary palate begins to form at about 35 days • complete lip development occurs by the 6th week, and palatal fusion follows • Cause of clefting defects: • mutations in single genes (TBX22, IRF6, MSX1) • chromosomal aneuploidy or deletion syndromes (trisomy 13, velocardiofacial syndrome) • teratogens (anticonvulsants) https://web.duke.edu/anatomy/embryology/craniofacial/craniofacial.html
Prenatal Diagnosis/Preparation Current Diagnosis: Orofacial Clefting
Embryology • Cleft palate occurs when the palatal shelves fail to fuse • Unilateral vs bilateral • vary in severity from submucous cleft to primary/secondary palates • Cleft lip occurs when there is interruption or hypoplasia of the mesenchymal layer • Unilateral vs bilateral • Small notch in the border of the lip vs. complete separation at the philtral column to border of the nose
Feeding • Difficulty creating seal and suctioning properly • Usually require supplementation/bottlefeeds vs. exclusively breastfeeding • Small, more frequent feeds • Upright position, increase burpings, squeezable bottles, plastic guard www.elroubyegypt.com
Cleft Lip Treatment • Nasoalveorlar Molding treatment (NAM): repositions the neonatal alveolar segments • brings the lip elements into close approximation • stretches the deficient nasal components • narrow width of cleft • After NAM, the definitive single-stage cleft lip and nose repair is performed at 3 to 6 months of age • With this initial operation, the lip/cleft deformity & nasal reconstruction
Cleft Palate Treatment • Cleft Palate repair: between 6-12 months of age • Benefit of better speech outcome, but poses the risk of impairing maxillary growth • Several techniques are used in CP repair: • Most common: Furlow double-opposing Z-plasty being the most common. • As they get older, children may need revisions of a cleft lip or palate repair, along with alveolar grafting or rhinoplasty to repair a nasal deformity associated with the cleft lip Markings for the Furlow double opposing Z-plasty palatoplasty
Complications • Feeding • Dehydration • Growth • Recurrent ear infections • Myringotomy tubes • Hearing loss • Dysfunctional speech and communication • Nasal voice • Pronounciation • Dental complications • Social: physical and emotional strain • Multiple surgeries • Emotional outcome
References • Samanich, J. “CleftPalate.” Pediatrics in Review: http://pedsinreview.aappublications.org/content/30/6/230.full.pdf+html • Bogdanow,A. Menasse-Palmer,L., Marion,R., Shaske,A. “CleftPalate.” Pediatrics in Review:http://pedsinreview.aappublications.org/content/16/11/424.full.pdf+html?sid=6caa0fe5-c22d-47ad-8b18-d5771f59e35b • Tolarova,M. “PediatricCleft Lip andPalate.” http://emedicine.medscape.com/article/995535-overview • Winchester, L. “Alveolar bone grafting: why and when?” http://www.clapa.com/medical/article/336/