Dermatomyositis and Scleroderma: Clinical Features and Treatment
840 likes | 953 Vues
Learn about the etiology, diagnosis, and treatment of dermatomyositis and scleroderma, including associated connective tissue diseases and autoimmune disorders. Understand the clinical manifestations, complications, and diagnostic tests for these conditions.

Dermatomyositis and Scleroderma: Clinical Features and Treatment
E N D
Presentation Transcript
Unit 5. Dermatomyositis,Scleroderma – Etiology, Clinical features, Diagnosis and Treatment. 1.5 hr Subacute cutaneous lupus erythematosus Discoid lupus erythematosus - Etiology, Clinical features, Diagnosis and Treatment. 0.5 hr
Connective Tissue Diseases(CTD)-concept • Autoimmune diseases– diseases associated with specific autoantibodies • Connective-tissue disorders— collagen-vascular disorders, are characterized by autoantibody-mediated connective-tissue abnormalities. • Histopathology: --Perivascular collagen deposition =Collagen Vascular Diseases • Symptoms nonspecific & overlapping
Connective Tissue Diseases(CTD) • Dermatomyositis • Scleroderma-Systemic Sclerosis-Diffuse Sclerosis* • Localized Fibrosing Disorders • - Linear Scleroderma • Morphea, & Regional Fibrosis • Lupus Erythematosus (LE): • Acute-, Subacute Cutaneous-LE, Discoid-LE, • Drug-Induced -, Bullous -, Systemic -,Neonatal - • Mixed Connective Tissue Disease, MCTD • Sjogren Syndrome • Eosinophilia-Myalgia Syndrome • Eosinophilic Fasciitis • CREST Syndrome
Definition of DM • an idiopathic inflammatory myopathy (IIM) with characteristic cutaneous changes • a systemic disorder that frequently affects the joints, esophagus, lungs, heart (rarely) • Related to Malignancy (>60y) • Calcinosis (in children, 40%) • Prognosis • Level of myopathy • y/n malignancy • Cardiopulmonary Involvment
Dermatomyositis-concept • Proximal muscle weakness nonsuppurative inflammation of skeletal muscle • 5 cases per million per year • 2:1 female:male • No racial disposition • Can occur at any age, 2 peaks • Adults – 50y(40-60) • Children – 5-15y
Cause & Pathophysiology of DM • Genetic – HLA DR3,DR5,DR7, TNF-a polymorphism • Immunologic abnormalities – antibody-mediated cell cytotoxicity vascular inflammation • Infectious – viral agents, Toxoplasma, Borrelia • Drug-induced – Hydrea, penicillamine, statin, quinidine, phenylbutazone • Silicone breast implants – anecdotal
Clinical features of DM • eruptions on exposed surfaces-- • as one of the initial manifestations • Muscle involvement – • manifests as proximal muscle weakness. • Systemic manifestations may occur • --arthralgia, arthritis, dyspnea, dysphagia, • arrhythmia, dysphonia
Clinical features of DMHallmark Skin lesion • the characteristic • a heliotrope discoloration on the upper eyelids • Gottron papules: violaceous, scaly papule-macule • nailfold telangiectasia • poikiloderma in a photodistribution. • Pruritic • Scaly scalp or hair loss Classic Cutaneous Manifestations
The heliotrope flower The heliotrope rash is a characteristic and pathognomonic cutaneous feature of DM.
Systemic Manifestations/Associations of Dermatomyositis/Polymyositis
Lung disease — • Interstitial lung disease (ILD) • is an important complication • may be associated with rapidly progressive • pulmonary failure and death • respiratory insufficiency • may result from diaphragmatic • and chest wall muscle weakness
Malignancy of DM • paraneoplastic processes • ---linked to oncogenesis & autoimmunity • Including: • Nasopharyngeal cancer • breast cancer lung cancer • pancreatic cancer colorectal cancer • ovarian cancer stomach cancer • cholangial canceresophageal cancer • laryngeal cancer liver cancer • tongue cancer renal cancer • Lymphoma
Complications • Cutaneous Ulceration • Systemic Vasculopathy • Calcinosis • Internal Malignancy • Opportunistic Infections and Lymphoma
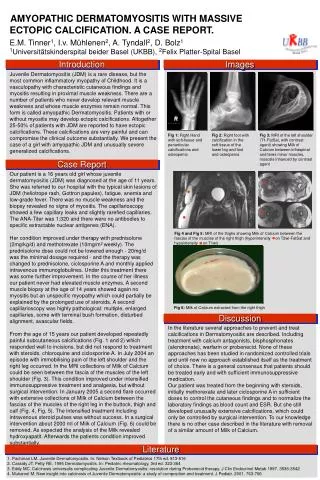
Amyopathic DM (ADM) • Typical cutaneous manifestations • No muscle symptoms • Normal muscle enzymes • Subclinical muscle disease • Px – mild proximal weakness • EMG – mildly abnormal • Abnormal US, MRI, Biopsy • new autoantibodies (140 kDa, 155 kDa, and Se) might serve as serologic markers • may reflect an underlying malignancy !
Laboratory Studies of DM • elevation of Muscle enzyme • creatine kinase(CK)level,aldolase level test • Aspartate aminotransferase(AST) • lactate dehydrogenase (LDH)tests • serologic abnormalities: • *ANA, • * three major categories of myositis-specific Abs (MSAs): • 1,Abs to aminoacyl-tRNA synthetases (antisynthetase Abs ) • including anti-Jo-1; • 2, Abs to signal recognition particle (anti-SRP Abs); • 3,Abs to Mi-2, a nuclear helicase. • *other myositis-specific autoantibodies
Imaging Studies Other tests • Pulmonary function studies • Electrocardiography (ECG) • skin biopsy • Muscle biopsy • MRI • Chest radiography • A barium swallow • Ultrasonography • Electromyography(EMG) • CT scanning
Histologic Findings Skin biopsy an interface dermatitis Muscle biopsy perivascular and interfascicular lymphocytic inflammation
perivascular and perimysial inflammation, & perifascicular necrosis.
Diagnosis of DM • Proximal muscle weakness • Elevated serum creatinine kinase • Myopathic changes on electromyography • Muscle biopsy with evidence of lymphocytic inflammation • Rashs(Gottron’s sign, heliotrope rash) • Positive auto-antibody:ANA,Jo-1
Differential Diagnoses CREST SyndromeParapsoriasisGraft Versus Host DiseasePityriasis Rubra PilarisLichen MyxedematosusPolymorphous Light EruptionLichen PlanusPsoriasis, PlaqueLupus Erythematosus, AcuteRosaceaLupus Erythematosus, DiscoidSarcoidosisLupus Erythematosus, Subacute CutaneousTinea CorporisMorpheaUrticaria, ChronicMulticentric Reticulohistiocytosis
Treatment of DM– general • difficult • Bed rest - in severe myopathy • Physical therapy - prevents curvatures in children, lasting joint damage (rare) • Elevate head after eating – prevent aspirations, may need NGT(nasogastric tube) • High protein diet
Treatment • photosensitive - sun avoidance and sun protective measures, sunscreens; Hydroxychloroquine, chloroquine • symptomatic patients:Steroids • non-responders:immunosuppressive agents methotrexate cyclosporine azathioprine tacrolimus fludarabine cyclophosphamide leflunomide chlorambucil mycophenolate mofetil • Anti-TNF agents (Infliximab) • Rituximab,anti-CD20 antibody specific in targeting the antibody-producing B cells • IVIG
Scleroderma-Background • Scleroderma is derived from the Greek words skleros (hard or indurated) and derma (skin) • Hippocrates first described this condition as thickened skin • 1752, Carlo Curzio offered the first detailed description of scleroderma in a patient with hard skin-- described as woodlike or containing a dry hide • 1836, Giovambattista Fantonetti applied the term scleroderma to a patient's condition--described as dark leather-like skin who exhibited a loss of range of joint motion due to skin tightening. • 1945, Robert H. Goetz first described the concept of scleroderma as a systemic disease-- he introduced the term progressive systemic sclerosis(PSS) to emphasize the systemic & often progressive nature of the disease
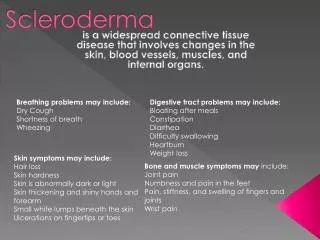
Sclerodermadefinition • a chronic multisystem disorder characterized by: --the overproduction & accumulation of collagen: **excessive fibrosisof the skin --with skin thickening &induration **fibrosis &chronic inflammatory infiltrationin organs --structural and functional abnormalities of blood vessels & organs --GI tract, lung, heart and kidneys **immune system activation (autoimmunity) **vasculopathy.
Environmental factors 1) silica dust 2) organic solvents 3) biogenic amines 4) urea formaldehyde 5) polyvinyl chloride 6) rapeseed oil 7) bleomycin 8) L-tryptophan 9) silicone implant (?) Genetic predisposition Defective immunoregulation 1) cell mediated immunity: CD4/CD8 , cytokines 2) humoral immunity hypergammaglobulinemia autoantibodyproduction antinuclear antibody (+) > 95% Etiology
Pathogenesis Susceptible host Exogenous events Immune system activation Endothelial cell activation/damage Fibroblast activation End stage pathology Obliterative vasculopathy Fibrosis
Pathogenesis • 1. Vasculopathy of small artery and capillary • - endothelial cell injury • - adhesion and activation of platelet • - PG F, thromboxane A2 release • - vasoconstriction & growth of endothelial cell and fibroblast • - narrowing or obliteration, increased permeability • 2. Fibrosis • - aberrant regulation of fibroblast cell growth • - increased production of extracellular matrix • (collagen, fibronectin, and glycosaminoglycan) • - thickening of the skin & fibrosis of internal organs
Classification 1. Systemic sclerosis (Scleroderma) • Diffuse cutaneous systemic sclerosis • Limitedcutaneous systemic sclerosis • Overlap syndromes 2. Localized scleroderma -Morphoea -Linear scleroderma 3. Overlap syndromes • Features of systemic sclerosis together with those of at least one other autoimmune disease, e.g. SLE, RA, or polymyositis
Clinical features of Scleroderma * CREST syndrome - calcinosis, Raynaud's phenomenon, esophagealdysmotility, sclerodactyly, telangiectasia
Clinical features ofScleroderma 1. Vascular abnormalities Vasculopathy 1) Raynaud's phenomenon - cold hands and feet • reversible skin color change (white to blue to red) • - induced by cold temperature or emotional stress • - initial complaint in 3/4 of patients • - 90% in patients with skin change • (prevalence in the general population: 4-15%) 2) digital ischemic injury
Clinical featuresScleroderma 2. Skin involvement (1) 1) stage-- - edematous phase - indurative phase - atrophic phase 2) firm, thickened bound to underlying soft tissue 3) decrease in range of motion loss of facial expressioninability to open mouth fully contractures
Clinical features 2. Skin involvement (2) ulceration loss of soft tissue of finger tip pigmentation calcific deposit 3. Musculoskeletal system Polyarthritis and flexion contracture Muscle weakness and atrophy (primary /secondary)
Terminal digit resorption Acrolysis Acrosclerosis
Calcinosis Calcinosis & acrolysis
Clinical features 4. gastrointestinal involvement 1) esophagus: hypomotility and retrosternal pain, reflux esophagitis, stricture 2) stomach: delayed emptying 3) small intestine: pseudo-obstruction, paralytic ileus malabsorption, weight loss, cachexia 4)large intestine: chronic constipation fecal impactiondiverticula
Clinical features 5. lungs 1) 2/3 of patients affected - leading cause of mortality and morbidity in later stage 2) pathology - interstitial fibrosis - intimal thickening of pulmonary arterioles (pulmonary hypertension) 3) Complains - dry cough breathlessness (Progressive dyspnea)
Clinical features 6. kidney 1) pathology - intimal hyperplasia of the interlobular artery - fibrinoid necrosis of afferent arterioles - glomerulosclerosis 2) proteinuria, abnormal sediment, azotemia, microangiopathic hemolytic anemia, renal failure
Clinical features 7. Cardiovascular system • Pericarditis,pericardial effusion,myocardial fibrosis --Congestive heart failure --Dyspnea • conduction abnormalities --arrhythmia (irregular heart beats) --Palpitations --syncope 8.Exocrine glands • Xerostomia • xerophthalmia
Laboratory findings 1. ANA, RF 2. anti-Scl-70 (DNA topoisomerase I) antibody • 20-40% in diffuse scleroderma • 10-15% in limited scleroderma 3. anticentromere antibody • 50-90% in limited scleroderma • 5% in diffuse scleroderma