Management of Non-Visible Haematuria in Adults: Guidelines for General Practitioners
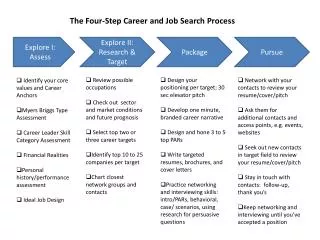
This guideline outlines the assessment and management of non-visible haematuria (NVH) in adults by general practitioners (GPs). It emphasizes the importance of urinalysis and initial investigations such as blood pressure measurement and eGFR. Special attention is given to persistent asymptomatic NVH in patients over 40 and those under 40 with cola-colored urine. Criteria for nephrological referral are specified, particularly regarding declining GFR and significant proteinuria. Ultimately, it provides a framework for secondary care management following a thorough evaluation.

Management of Non-Visible Haematuria in Adults: Guidelines for General Practitioners
E N D
Presentation Transcript
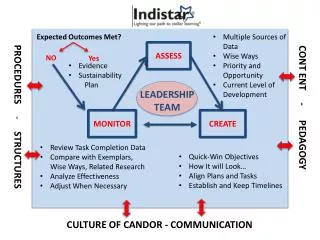
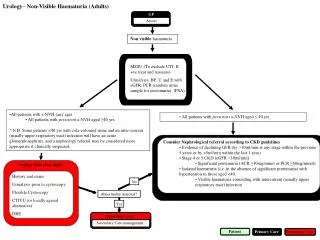
Urology – Non-Visible Haematuria (Adults) GP Assess Nonvisible haematuria MSSU (To exclude UTI, If +ve treat and reassess) Urinalysis, BP, U and E with eGFR, PCR (random urine sample for proteinuria). (PSA) • All patients with s-NVH (any age). • • All patients with persistent a-NVH aged ≥40 yrs. • * N.B. Some patients <40 yrs with cola-coloured urine and an inter-current (usually upper respiratory tract) infection will have an acute glomerulonephritis, and a nephrology referral may be considered more appropriate if clinically suspected. • • All patients with persistent a-NVH aged ≤ 40 yrs. • Consider Nephrological referral according to CKD guidelines • • Evidence of declining GFR (by >10ml/min at any stage within the previous 5 years or by >5ml/min within the last 1 year) • • Stage 4 or 5 CKD (eGFR <30ml/min) • • Significant proteinuria (ACR ≥30mg/mmol or PCR ≥50mg/mmol) • • Isolated haematuria (i.e. in the absence of significant proteinuria) with hypertension in those aged <40. • • Visible haematuria coinciding with intercurrent (usually upper respiratory tract) infection Urology One stop clinic History and exam Urinalysis prior to cystoscopy Flexible Cystoscopy CTIVU (or locally agreed alternative) DRE No Abnormality detected? Yes Secondary Care Secondary Care management Patient Primary Care Secondary Care