Download
1 / 68
780 likes | 1.21k Vues
LESSON 20. PREGNANCY AND CHILDBIRTH. Introduction. Childbirth sometimes occurs outside planned setting Delivery rarely becomes medical emergency Medical problems or complications can become emergencies. Pregnancy and Labor. Begins with fertilization of ovum

E N D
LESSON 20 PREGNANCY AND CHILDBIRTH
Introduction • Childbirth sometimes occurs outside planned setting • Delivery rarely becomes medical emergency • Medical problems or complications can become emergencies
Pregnancy and Labor • Begins with fertilization of ovum • Growth and development proceed over 40 weeks
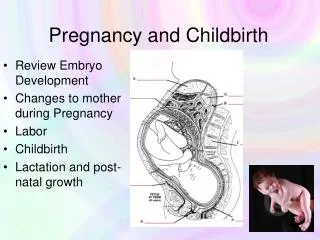
Stages of Pregnancy • Divided into 3 trimesters – 3 months each • Single cell divides into many • First 8 weeks is an embryo; then a fetus • Embryo attached to placenta • Fetus develops inside amniotic sac • All major organ systems developed by week 8
Fetus fully formed by week 36 Near end of pregnancy, head of fetus positioned downward in pelvis Fetus passes through dilated cervix and vagina Stages of Pregnancy (continued)
Stages of Labor and Delivery • “Show” or “bloody show” may occur before labor begins • When mucus plug from cervix released • Can occur up to 10 days before contractions begin • Labor and delivery occurs in 3 stages beginning with contractions
Stage 1: Labor to Cervical Dilation • Amniotic sac ruptures before or during first stage • Uterine contractions begin and eventually push infant’s head into cervix • 10-15 minutes apart initially • 2-3 minutes apart shortly before birth • May last few hours to a day
Stage 2: Delivery • Typically lasts 1-2 hours • Cervix fully dilated • Contractions powerful and painful • Infant’s head presses on floor of pelvis – woman has urge to push down • Vagina stretches open • Head emerges (crowning) • Rest of body pushed out
Placenta separates from uterus and delivered –usually within 30 minutes of birth Uterus contracts and seals off blood vessels Stage 3: Childbirth to Placenta Delivery
Emergency Care During Pregnancy • Women who receive regular care are advised about potential problems to watch for • Although rare, problems may require emergency care
Vaginal Bleeding • Light irregular discharges of a small amount of blood (spotting) may be normal • Vaginal bleeding during pregnancy is abnormal • May be caused by cervical growths or erosion, problem with placenta or miscarriage • In third trimester may be sign of preterm birth • See health care provider immediately
Assessing Vaginal Bleeding • Perform standard assessment • Assess for pain and any signs of shock • Take repeated vital signs • The history should include an obstetric history
Emergency Care forVaginal Bleeding • Perform standard patient care • Have female assistant present if possible • Position patient lying on left side • Don’t control bleeding by keeping patient’s legs together • Give patient towel or sanitary napkins
Emergency Care forVaginal Bleeding (continued) • Don’t try to pack vagina • Save expelled material to give to arriving EMS • Follow local protocol re: oxygen administration • Treat for shock • Provide emotional support
Miscarriage • Loss of embryo or fetus in first 14 weeks • 10% 25% of pregnancies end in a miscarriage • May result from: • Genetic disorder • Fetal abnormality • Factor related to woman’s health • No known cause • Most women don’t have problems with later pregnancies
Assessing Miscarriage • Perform standard assessment • Take repeated vital signs
Signs and Symptoms of Miscarriage • Vaginal bleeding • Abdominal pain or cramping
Emergency Care for Miscarriage • Provide same emergency care as vaginal bleeding in pregnancy • Retain expelled materials for EMS personnel • Be calm and reassuring
Trauma in Pregnancy • Woman’s blood volume increases significantly in pregnancy • Blood loss may not immediately cause signs of shock • Blood flow reduced to fetus • Signs of internal blood loss may not be apparent
Emergency Care for Trauma in Pregnancy • Perform standard patient care • Assume there may be internal bleeding • Treat for shock • Follow local protocol for oxygen administration • Don’t let patient late in pregnancy lie flat on her back • Raise right side higher to reduce pressure on vena cava
Other Problems in Pregnancy See health care provider if you have: • Abdominal pain • Persistent or severe headache (sign of toxemia) • Sudden leaking of water • Persistent vomiting, chills and fever, convulsions, difficulty breathing • Persistently elevated blood pressure • Signs or symptoms related to diabetes
Childbirth • Remember it is a natural process • Woman may be fearful or distressed • Remain calm
Supportive Care During Labor • Ensure plan for transport • Help woman rest • Provide comfort measures • Do not let woman have bath • Write down contraction intervals and length • Remind woman to control breathing • Continue to provide reassurance
Assessing Whether Delivery Is Imminent • Labor usually lasts for several hours • In rare occasions, labor progresses quickly • May begin weeks before due date • Prepare to assist in childbirth if delivery may be imminent • Braxton Hicks contractions do not signal beginning of labor, but do not assume woman is not in labor when she feels contractions
Gather Information from the Woman • Name, age and due date • Physician’s name and telephone number • Ask if she: • Has given birth before • Knows whether she may be having twins • Has broken her water and to describe it • Has experienced any bleeding • Has any past or present medical problems • Give this information to arriving EMS personnel
Assessing Childbirth Imminence • Has the “bloody show” occurred? • When did contractions begin? • How close together are they? • How long does each last? • When contractions are about 2 minutes apart, delivery will likely occur very soon • Feels strong urge to push? • Check whether infant’s head is crowning
Preparing for Delivery • Someone must stay with woman • Gather the items needed or helpful for delivery • Many EMRs carry obstetrics kit
Items Needed for Delivery • Clean blanket or coverlet • Several pillows • Plastic sheet or stack of newspapers (to cover bed surface) • Clean towels and washcloths • Sanitary napkins or pads of clean cloth • Medical examination gloves • Basin and plastic bags (for afterbirth) • Medical hazard bag or designated plastic bag (for clean-up)
Items Needed for Delivery (continued) • Bowl of hot water (for washing but not the infant) • Empty bowl (in case of vomiting) • Clean handkerchief (to wear as facemask) • Clean, soft towel, sheet or blanket (to wrap newborn) • Eye and face protection for yourself, if available • Oxygen if available • Bulb syringe (to suction infant’s mouth)
Items Needed for Delivery (continued) If help may be delayed: • Clean strong string, shoelaces or cloth strips (to tie cord) • Sharp scissors, knife or razor (to cut cord) • Sterilize first in boiling water for 5 minutes • Or sterilize by holding over flame for 30 seconds
Preparation for Childbirth • Provide privacy for the mother • Prepare birthing bed • Roll up sleeves, wash hands thoroughly for 5 minutes, put on medical examination gloves • Protect your eyes, mouth and nose from blood and other fluids
Preparation for Childbirth (continued) • Do not let woman use bathroom • Do not touch vaginal areas except during delivery • Call dispatch or health care provider for additional instructions • Do not make an internal vaginal examination • When crowning occurs, move woman into birthing position • Assist with delivery
Help woman lie on back with knees bent and apart and feet flat
As infant’s head appears, have gloved hands ready to receive and support the head
As the head emerges (usually face down), support the head • After the head is out, have the woman stop pushing and breathe in a panting manner
Hold infant with head lower than feet • Suction nose and mouth with bulb syringe
Gently dry and wrap the infant in a towel or blanket to prevent heat loss, keeping the cord loose • Follow your local protocol to clamp or tie the umbilical cord or leave it intact for arriving EMS personnel
Wait for delivery of afterbirth, placenta and umbilical cord – do not pull on umbilical cord in an attempt to pull out placenta • Continue to monitor both mother and newborn
Care of the Mother After Delivery • Support and comfort mother • Monitor pulse and breathing • Replace any blood-soaked sheets or blankets, dispose of used supplies • Mother may drink water now
Bleeding After Delivery • Somebleeding normally occurs with childbirth and delivery of placenta • Usually stops after placenta is delivered • Use sanitary pads or clean folded cloths to absorb blood
Care for BleedingAfter Delivery To help stop bleeding, massage abdomen below navel with a continuous circular motion • Be sure you are kneading with your palms • Keep mother still and try to calm her • Treat for shock • Follow local protocol for oxygen administration • Encourage breastfeeding
Assess the Newborn • Note skin color, movement and whether crying is strong or weak • Normal respiratory rate is more than 40 breaths/minute • The normal pulse is more than 100 beats/minute • Note any changes over time • Provide this information EMS personnel
Care of the Newborn (continued) • Dry newborn • Ensure infant stays wrapped, including the head, to stay warm • Support newborn’s head if it must be moved for any reason • Continue to check breathing and airway