Download
1 / 104
1.05k likes | 1.23k Vues
1,5 Anhydroglucitol and the Monitoring of Postprandial Glucose Control. Steven D Wittlin M.D. U of Rochester School of Medicine and Dentistry. Importance of Post-Prandial Hyperglycemia. Breakfast. Dinner. 0:00 am. 4:00 am. Breakfast. Lunch. Postprandial.

E N D
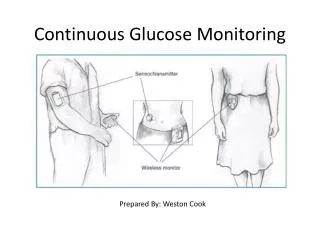
1,5 Anhydroglucitol and the Monitoring of Postprandial Glucose Control Steven D Wittlin M.D. U of Rochester School of Medicine and Dentistry
Breakfast Dinner 0:00 am 4:00 am Breakfast Lunch Postprandial Duration of daily metabolic conditions Postabsorptive Fasting Monnier L. Eur J Clin Invest 2000;30(Suppl. 2):3–11
r=0.97 Correlation between plasma glucose levels after OGTT and standard mixed meal Wolever TMS et al. Diabetes Care 1998;21:336–40
Relationship between HbA1C, FPG and 2 h. PPG Van Haeften T et al Metabolism 2000
Relative Changes in FPG and 2-h PG as HbA1c Increases 250 = HbA1c versus 2hppg = HbA1c versus FPG Plasma Glucose (mg/dL) 160 r = 0.55 y = 47.1 x -109 r = 0.48 y = 12.0 x +30 70 4 5 6 7 HbA1c (%) Woerle HJ et al Arch Intern Med. 2004;164:1627-1632.
Relationship between FPG and 1st-Phase Insulin Release( van Haeften T et al Metabolism 2000 )
Relationship Between Diabetes Status and 1st Phase Insulin Release( van Haeften T et al .Metabolism 2000 )
As Patients Get Closer to A1C Goal, the Need to Successfully Manage PPG Significantly Increases Adapted from Monnier L, Lapinski H, Collette C. Contributions of fasting and postprandial plasnma glucose increments to the overall diurnal hyper glycemia of Type 2 diabetic patients: variations with increasing levels of HBA(1c).Diabetes Care. 2003;26:881-885.
Age 0.21* 0.25* Body mass index (BMI) 0.01 0.24* Waist: hip ratio 0.15 0.21* Triglycerides 0.01 0.23* Free fatty acids 0.07 0.27‡ Tissue plasminogen activator (TPA) 0.18 0.25‡ Cellular fibronectin –0.03 0.25‡ C-reactive protein –0.13 0.20* Post-load Hyperglycemia and The Metabolic Syndrome Fasting plasma glucose 2-hr plasma glucose *p<0.05; ‡ p<0.01 Yudkin JS. Lancet 2002;359:166–7
Controlling Postprandial Glucose • Prospective trial of fasting vs pc control in 164 pts w/ Type 2 DM • Forced titration to target first FBS < 100 and then, 90 min pc < 140 if not achieved previously • Results: • HbA1C fell from 8.7 % to 6.5% • Only 64% of patients achieving FPG < 100 only reached HbA1C < 7% • 94% of patients w/ pc < 140 reached HbA1C < 7% • Decreased pc BG accounted nearly twice as much as FBS for fall in HbA1C • If HbA1C < 6.2% , pc accounted for ~ 90% • If HbA1C > 8.9%, pc accounted for ~ 40% Woerle HJ et al Diabetes Research and Clinical Practice 2007
Contribution of Postprandial BG to HbA1C Woerle HJ et al Diabetes Res Clin Pract. 2007 Jan 19
Glycemic Excursions Predict Oxidative Stress Monnier L et al JAMA. 2006;295:1681-1687
Endogenous Glucose Production After a Mixed Meal in Diabetic and Non-Diabetic Individuals(Singhal P et al AJP 2002 )
Post-Prandial Glucose Metabolism : Mechanism • Study of 11 normal volunteers after a standard test meal • Triple isotope technique and indirect calorimetry • Intravenous • Tritiated Glucose • C-14-labelled bicarbonate • Oral • Deuterated Glucose Woerle HJ et al .Am J Physiol Endocrinol Metab 284: E716-E725, 2003
Post-Prandial Glucose Disposal ( Woerle Hans J et al AJP Endo Metab 2003 )
Changes in Postprandial Glucose Metabolism in Type 2 DM • Use triple isotope technique and indirect calorimetry • DM pts had: • increased overall glucose release • Increased gluconeogenesis and glycogenolysis • ~90% of the increased glucose release occurred in the first 90 min post-prandial • In DM glucose clearance and oxidation were reduced • Non-oxidative glycolysis was increased • Net splanchnic glucose storage was reduced ~ 45% d.t. increased glycogen cycling Woerle HJ et al Am J Physiol Endocrinol Metab 2006
Effect of Pre- or Post-Meal Exercise on Glycemic Control(Yamanouchi K et al Diab Res & Clin Pract, Oct 2002 )
Effects of 2h Post-Prandial Glucose +/- Vitamins C +E on Flow-Mediated Dilatation( Title LM et al JACC Dec 2000 )
Relative risk for death increases with 2-hour blood glucose irrespective of the FPG level 2.5 2.0 1.5 1.0 0.5 0.0 Hazard ratio ³11.1 7.8–11.0 2-hour plasma glucose(mmol/l) <7.8 <6.1 6.1–6.9 ³7.0 Fasting plasma glucose (mmol/l) Adjusted for age, center, sex DECODE Study Group. Lancet 1999;354:617–621
Effect of Acarbose on CVD in Patients with IGT ( STOP-NIDDM)( Chiasson J-L et al JAMA July 2003 )
Summary • Postprandial glycemia plays a clinically important role in the complications of diabetes • Postprandial glycemia is a major contributor to overall glycemic control ESPECIALLY in moderately-well to well controlled patients
So How Can We Assess Post-Prandial Glucose Control Clinically ?? • Frequent fingersticks • HbA1C • Fructosamine • Continuous Glucose Monitoring Systems • Historical • Real-time • 1,5 Anhydroglucitol
A New Idea ! 1,5 Anhydroglucitol
History of 1,5AG 1888 1,5AG was discovered in plant of Polygala Senega. 1973 Presence in human body was reported. 1977 Decrease of plasma 1,5AG concentration with uremia and diabetes mellitus was reported. 1979 Blood 1,5AG was determined in Japan. After this, research on relationship between diabetes mellitus and 1,5AG has become active.
Blood test measuring 1,5-anhydroglucitol (1,5-AG) 1,5-AG is a monosaccharide (similar to glucose structure) 1/40 of glucose concentration – healthy human blood Primary Source of 1,5-AG – Food Further distributed to skin, muscle, and other tissues/organs Reabsorbed very efficiently through kidney (urinary excretion is 1/20 of total amount in body) Large Body Pool of 1,5-AG (6-7 times > Blood) Not metabolized much in the body (metabolic turnaround rate at least 3 days) 1,5-AG urinary excretion remarkably increases with hyperglycemia!
HO HO O O OH OH OH HO HO OH OH The structure of 1,5-anhydroglucitol (1,5AG) D-glucose 1,5-anhydro-D-glucitol ((1-deoxyglucose)
Fully Automated Enzymatic Method for 1,5 AG Assay ( Glycomark ) Fukumura Y et al Clin Chem 1994 HRP=Horseradish peroxidase ; PROD= pyranose oxidase; HTB=3 hydroxyriiodobenzoic acid ; 4AAP= 4 aminoantipyrine
Specificity of Assay • The following don’t interfere in concentrations up to 10 grams/L : • Sorbitol • Mannitol • Sucrose • Lactose • Maltose • Fructose
1,5 AG Content of Foodstuffs in Japanese Diet Yamanouchi T et al Am J Physiol 263: E268-E273. 1992
Physiology of 1,5-AG Oral Supply 1,5AG (5-10mg/day) A. Normoglycemia Oral Supply 1,5AG (5-10mg/day) B. Hyperglycemia Tissues Internal Organs (500- 1000 mg) Tissues Internal Organs (500- 1000 mg) Blood Stream (1,5-AG Level Lower) Blood stream Glucose Blocks Reabsorption Kidney Kidney Urinary excretion (INCREASED) Urinary excretion (5-10mg/day) Buse JB et al Diab Tech & Ther 2003. 5(3) : 355-363
1,5 AG Kinetics in Humans Yamanouchi T et al Am J Physiol 263: E268-E273. 1992
Urinary Excretion of Glucose and 1,5 AG Fluctuate in Parallel in Rats Yamanouchi T et al Am J Physio 1990. 258: E423-E427
Urinary Excretion of Glucose and 1,5 AG Fluctuate in Parallel in Rats Yamanouchi T et al Am J Physio 1990. 258: E423-E427
But…1,5 AG Does Not Fluctuate with Variations in Plasma BG in Nephrectomized Rats !! Yamanouchi T et al Am J Physio 1990. 258: E423-E427
Fructose , Mannose and 1,5 AG Share A Common Transport Mechanism Yamanouchi T et al Biochim et Bipophys Acta 1996. 1291: 89-95
Fructose , Mannose and 1,5 AG Share A Common Transport Mechanism Yamanouchi T et al Biochim et Bipophys Acta 1996. 1291: 89-95
Renal Tubular Absorption of Glucose and 1,5 AG Normal Filtration atglomerulus Glucose active transporter Fructose, mannoseactive transporter Glucose 1,5AG Reabsorption atrenal tubule urine
Renal Tubular Absorption of Glucose and 1,5 AG Hyperglycemia Filtration atglomerulus Reabsorption atrenal tubule Glucose active transporter Fructose, mannoseactive transporter Glucose 1,5AG urine
Renal Tubular Absorption of Glucose and 1,5 AG Stickle D and Turk J. Am J Physiol Endocrinol Metab 273: E821-E830, 1997
Linearity of 1,5 AG Assay Nowatzke W et al Clin Chim Acta 2004
Recovery Time of 1,5 AG in Treated Patients with Type 2 DM Yamanouchi T et al Jpn. J. Clin. Med. 47: 2472-2476, 1989
Male (n=332) Female (n=207) 50 50 40 40 21.5±6.0 26.6±7.2 30 30 Frequency Frequency 20 20 10 10 0 0 10 20 30 40 50 10 20 30 40 50 10 20 30 40 50 1,5AG (µg/mL) 1,5AG (µg/mL) 1,5AG (µg/mL) Male and Female (n=539) 70 60 24.6±7.2 50 40 Frequency 30 20 10 0 Histograms of serum 1,5AG concentrations in Japanese healthy subjects
Distribution of 1,5 AG in a Healthy US Population Nowatzke W et al Clin Chim Acta 2004
mean±SD The mean 1,5AG levels in healthy subjects during 2 years (n=245)
↑B ↑L ↑D ▲―▲: healthy ◆―◆:IGT Others: diabetes B: breakfast L: lunch D: dinner Diurnal change of plasma glucose and 1,5AG