Download
1 / 21
210 likes | 330 Vues
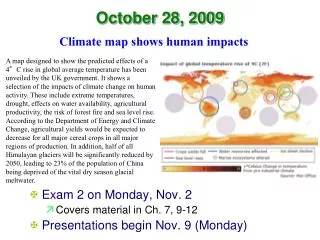
Producing and Measuring Quality Health Care For At Risk Kids Wisconsin Children’s Public Policy Forum Nikki Highsmith Center for Health Care Strategies. October 28, 2005. Impetus for Change. We Get the Right Care…About ½ of the Time.

E N D
Producing and Measuring Quality Health Care For At Risk Kids Wisconsin Children’s Public Policy Forum Nikki Highsmith Center for Health Care Strategies October 28, 2005
We Get the Right Care…About ½ of the Time Adherence to Processes Defined as Quality Indicators, By Type of Care Source: McGlynn, et at., NEJM, 2003
Impetus for Change:A Medicaid Growth Scenario Beneficiaries Expenditures $600B 75M 53M $329B 36M $133B 2005 2015 1995 2015 2005 1995
Medicaid’s Growth…The Reasons Why • Underlying growth in medical costs • Longevity increases for elderly and people with disabilities and/or with chronic diseases • Public coverage expansions (e.g., SCHIP) • Private coverage decimations (e.g., crowd-in)
Medicaid Spending Growth Compared to Private Spending (Holahan, 2005) 12.6% 9.0% 6.9% Health Care Spending Per Person with Private Coverage Monthly Premiums for ESI Medicaid Acute Care Spending Per Enrollee
Medicaid: Chaos or Opportunity? • Big Numbers • 52 million people • $320 billion in spending • Key Challenges • Disproportionate racial and ethnic participation • 80/20 • Increasingly Sophisticated Players • State Purchasers • Managed Care Entities (MCOs, EPCCM) • Safety Net Providers
Five Steps for Reducing Medicaid $$ HIGH Level of Difficulty LOW
Care Management Trends in Medicaid Opportunities • Create a medical home • Coordinate/create a continuum of care • Improve health outcomes/control costs Challenges • Choosing a model (HMO, e-PCCM, DMO) • Communication among interdisciplinary team • Managing care vs. managing cost
Care Management Trends: Moving Away from FFS All but three states enroll their members into RBMC, PCCM, or both.* # States (50 + DC) *Trend data adapted from: Kaye, Neva . "Medicaid Managed Care Looking Forward Looking Back." 2005. National Academy for State Health Policy . 08 Jul. 2005 <NASHP.org>.
Care Management Trends: Moving Into More Complex Populations Since 1994 over half of all states have enrolled some people with complex needs into a care management model. # States (50 + DC) *Trend data adapted from: Kaye, Neva . "Medicaid Managed Care Looking Forward Looking Back." 2005. National Academy for State Health Policy . 08 Jul. 2005 <NASHP.org>.
Evidence-Based Practices Opportunities • Incorporate scientific evidence into practice • Focus on single diseases (e.g. asthma, diabetes) • Emerging evidence (e.g. dental care) Challenges • Getting research into practice at state, plan, and provider level • Developing evidence/protocols for treating people with multiple chronic conditions and disabilities
Pay for Performance Opportunities • Use measures and payment system to align incentives to improve quality • Coordinate measures across P4P programs and across payors Challenges • Little research to date on design and effectiveness • Paying for “what they should be doing anyway” • Physician concerns re “demoralization” of field
Quality Improvement Opportunities • Implement quality improvement collaboratives to drive outcomes • Use of Best Clinical and Administrative Practices (BCAP) model to design and evaluate programs Challenges • Can be resource intensive • Needs continued and committed leadership on all levels
Monroe Health Plan of New York Analysis of NY State SPARCS Data Demonstrated No Concurrent Changes in NICU Admission Rates in Upstate New York for Medicaid During These Years
Developing the Return on Investment (ROI) Does Any of This Make a Difference? Ratio: (Pre-Program Medical Costs) – (Post-Program Medical Costs) Program Costs $3,565,688 = 2.86 $1,246,207
Developing the Business Case for Quality in Medicaid • Business Case = direct ROI for Quality Enhancing Initiative (QEI) • Plan A’s asthma QEI with practice site IT reduces ED use by $10 PMPM over 3-year period. • Economic Case = ROI $ for other Medicaid stakeholders • Plan A’s QEI reduces PMPM for other payors when patient churns elsewhere. • Social Case = broader benefits to society • Plan A’s QEI increases school/work attendance, quality of life, etc. Message: we need to find the “win-wins” and align financial incentives to reward quality.
Score-ability and the Long-term Business Case • OMB/CBO methods for scoring need to be changed. For example…maintaining electronic medical records, “would save the Feds billions and save lives as well”…however federal scorers only count the costs of launching the technologies and not the amount that would be saved over time. Newt Gingrich and Peter Ferrara Wall Street Journal September 26, 2005