Download
1 / 1
10 likes | 131 Vues
Tenofovir-Based Regimens for Non-Occupational Post-Exposure Prophylaxis (NPEP): Improved Tolerability and Adherence Compared to AZT-Based Regimens Kenneth H. Mayer 1, 2 , Matthew J. Mimiaga 1, 3 , Dan Cohen 1 , Chris Grasso 1 , Ronn Bill 1 , Rodney VanDerwarker 1, 4 , and Alvan Fisher 5

E N D
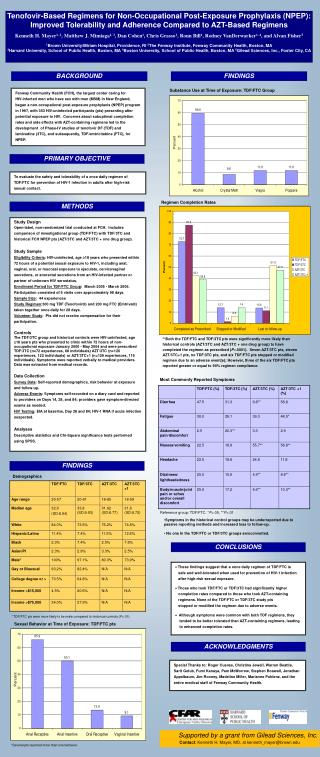
Tenofovir-Based Regimens for Non-Occupational Post-Exposure Prophylaxis (NPEP): Improved Tolerability and Adherence Compared to AZT-Based Regimens Kenneth H. Mayer1, 2, Matthew J. Mimiaga1, 3, Dan Cohen1, Chris Grasso1, Ronn Bill1, Rodney VanDerwarker1, 4, and Alvan Fisher5 1Brown University/Miriam Hospital, Providence, RI 2The Fenway Institute, Fenway Community Health, Boston, MA 3Harvard University, School of Public Health, Boston, MA 4Boston University, School of Public Health, Boston, MA 5Gilead Sciences, Inc., Foster City, CA BACKGROUND FINDINGS Substance Use at Time of Exposure: TDF/FTC Group Fenway Community Health (FCH), the largest center caring for HIV-infected men who have sex with men (MSM) in New England, began a non-occupational post-exposure prophylaxis (NPEP) program in 1997, with 353 HIV-uninfected participants (pts) presenting after potential exposure to HIV. Concerns about suboptimal completion rates and side effects with AZT-containing regimens led to the development of Phase-IV studies of tenofovir DF (TDF) and lamivudine (3TC), and subsequently, TDF/emtricitabine (FTC), for NPEP. PRIMARY OBJECTIVE * To evaluate the safety and tolerability of a once daily regimen of TDF/FTC for prevention of HIV-1 infection in adults after high-risk sexual contact. Regimen Completion Rates METHODS Regimen Completion Rates Study Design Open-label, non-randomized trial conducted at FCH. Includes comparison of investigational group (TDF/FTC) with TDF/3TC and historical FCH NPEP pts (AZT/3TC and AZT/3TC + one drug group). Study Sample Eligibility Criteria: HIV-uninfected, age 18 years who presented within 72 hours of a potential sexual exposure to HIV-1, including anal, vaginal, oral, or mucosal exposure to ejaculate, cervicovaginal secretions, or anorectal secretions from an HIV-infected partner or partner of unknown HIV serostatus. Enrollment Period for TDF/FTC Group: March 2005 - March 2006. Participation consisted of 6 visits over approximately 98 days. Sample Size: 44 experiences Study Regimen:300 mg TDF (Tenofovir) and 200 mg FTC (Emtriva) taken together once daily for 28 days. Volunteer Study: Pts did not receive compensation for their participation. Controls The TDF/3TC group and historical controls were HIV-uninfected, age 18 years pts who presented to clinic within 72 hours of non-occupational exposure January 2000 - May 2004 and were prescribed TDF/3TC (n=72 experiences, 68 individuals) AZT/3TC (n=126 experiences, 122 individuals) or AZT/3TC+1 (n=129 experiences, 119 individuals). Symptoms were reported verbally to medical providers. Data was extracted from medical records. Data Collection Survey Data: Self-reported demographics, risk behavior at exposure and follow-up. Adverse Events: Symptoms self-recorded on a diary card and reported to providers on Days 14, 28, and 84; providers gave symptom-directed exams as needed. HIV Testing: EIA at baseline, Day 28 and 84; HIV-1 RNA if acute infection suspected. Analyses Descriptive statistics and Chi-Square significance tests performed using SPSS. **Both the TDF/FTC and TDF/3TC pts were significantly more likely than historical controls (AZT/3TC and AZT/3TC + one drug group) to have completed the regimen as prescribed (P<.0001). Seven AZT/3TC pts, eleven AZT/3TC+1 pts, no TDF/3TC pts, and six TDF/FTC pts stopped or modified regimen due to an adverse event(s); However, three of the six TDF/FTC pts reported greater or equal to 90% regimen compliance. Most Commonly Reported Symptoms FINDINGS Demographics Reference group: TDF/FTC. *P<.05, **P<.01 • Symptoms in the historical control groups may be underreported due to passive reporting methods and increased loss to follow-up. • No one In the TDF/FTC or TDF/3TC groups seroconverted. CONCLUSIONS • These findings suggest that a once daily regimen of TDF/FTC is safe and well-tolerated when used for prevention of HIV-1 infection after high-risk sexual exposure. • Those who took TDF/FTC or TDF/3TC had significantly higher completion rates compared to those who took AZT-containing regimens. None of the TDF/FTC or TDF/3TC study pts stopped or modified the regimen due to adverse events. • Although symptoms were common with both TDF regimens, they tended to be better tolerated than AZT-containing regimens, leading to enhanced completion rates. * TDF/FTC pts were more likely to be male compared to historical controls (P<.01) Sexual Behavior at Time of Exposure: TDF/FTC pts ACKNOWLEDGMENTS Special Thanks to: Roger Cuevas, Christina Jewell, Warren Beattie, Sarit Golub, Fumi Kanaya, Pam McMorrow, Stephen Boswell, Jonathan Appelbaum, Jim Rooney, Madeline Miller, Marianne Poblenz, and the entire medical staff of Fenway Community Health. Supported by a grant from Gilead Sciences, Inc. Contact: Kenneth H. Mayer, MD, at kenneth_mayer@brown.edu *Several pts reported more than one behavior.