Download
1 / 13
220 likes | 1.2k Vues
Paravertebral block: a simple block to achieve somatic and sympathetic neural blockade of multiple dermatomes.. Clinical applicationsAnalgesia for:- thoracic surgery - upper abdominal surgery e.g. cholecystectomy - breast surgery - fractured ribs or contusions of the thoracic wall - upper leg surgery - .

E N D
1. PARAVERTEBRAL BLOCK- an underused block. Dr Mahesh Shah
The General Infirmary at Leeds
U.K.
3. Clinical applications
Analgesia for:- thoracic surgery
- upper abdominal surgery e.g. cholecystectomy
- breast surgery
- fractured ribs or contusions of the thoracic wall
- upper leg surgery
-
4. Clinical applications:- posthoracotomy and postmastectomy pain
- acute herpes zoster
- pain in the intercostal area e.g. causalgia or neuralgia.
5. Anatomy of the thoracic paravertebral space:
The paravertebral space is a wedge shaped compartment bounded by:
Above and below � heads and necks of the adjoining ribs
Posterior � costo-tranverse ligaments
Medially � communicates with the extradural space through the intevertebral
Laterally � bound by the parietal pleura with the apex leading into the intercostals space
The base � formed by the posterolateral aspect of the body of the vertebra and the intervertebral foramen
The upper aspect of the spinous process coincides with the transverse process of the lower vertebra
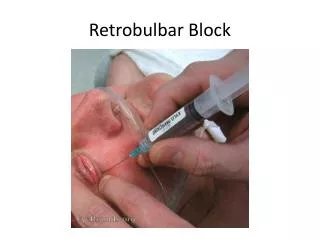
6. Technique of Thoracic paravertebral block.
The patient can be sitting, lateral or prone. The sitting position is the easiest. The needle is inserted 3cm lateral to the most cephalad portion of the spinous process and advanced at right angle to all skin planes to contact the transverse process of the vertebra below ( 2-4cm depth).
It is then redirected cephalad and advanced (1-1.5cm) till a loss of resistance is felt. A single injection of 15-20ml causes a blockade of 4 to 5 dermatomes with a tendency to caudal spread.
Multiple injections can be performed.
7. Anatomy of Lumbar paravertebrals:
Lumbar nerves exit the vertebral foramina inferior to the caudad edge of the transverse process. The anterior branches of L1 to L4 with a contribution from T12 form the lumbar plexus.
The cephalad aspect of the spinous process coincides with the caudad aspect of the homologous transverse process.
10. Technique of Lumbar paravertebral block
The patient is placed prone or lateral. At a point 3cm lateral to the cephalad edge of the spinous process the needle is inserted at right angles in all planes till it contacts the caudad aspect of the homologous transverse process.
The needle is then redirected off the caudad edge till a loss of resistance is felt and an impulse obtained with a nerve stimulator or paraesthesia is felt.
11.
Continuous catheter techniques can be used
12. Complications Local anaesthetic toxicity
Pneumothorax <1%
Epidural diffusion 1%
Hypotension <5%
Intravascular injection into the vena cava or aorta is possible.
13. Conclusion
The paravertebral block is an underused block with a low risk of complications.
It is easy to learn and use in clinical practice.