Failed Eye Exam
Failed Eye Exam. Rochelle Cochrane, M.D. January 13, 2006 Tracy Crnic, M.D. Case Presentation. 5 y/o Caucasian Female presents to pediatric ophthalmology clinic after “failing” school eye exam Mother has not noticed any eye problems up to this point. Pt has had normal development.

Failed Eye Exam
E N D
Presentation Transcript
Failed Eye Exam Rochelle Cochrane, M.D. January 13, 2006 Tracy Crnic, M.D.
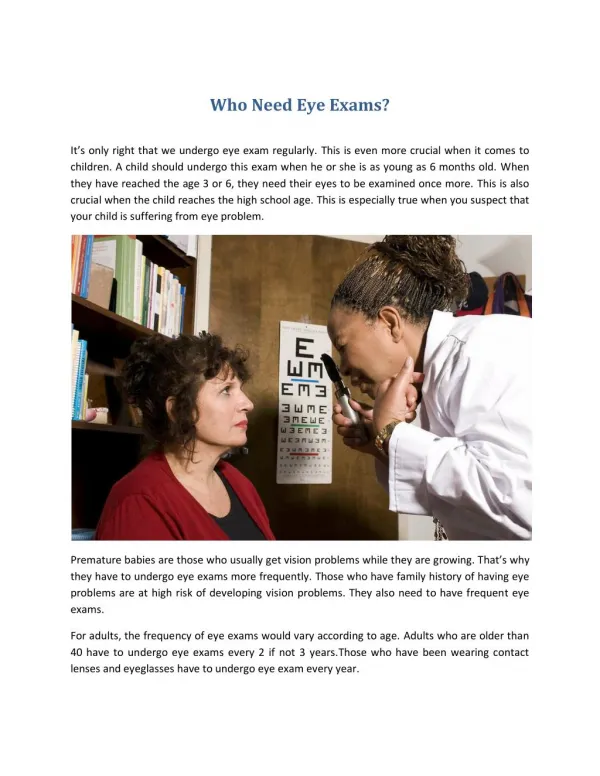
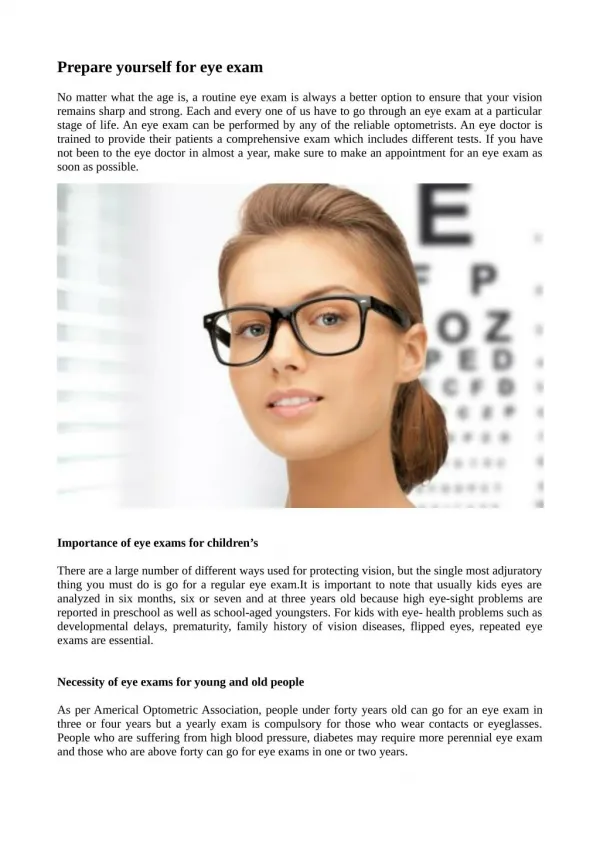
Case Presentation • 5 y/o Caucasian Female presents to pediatric ophthalmology clinic after “failing” school eye exam • Mother has not noticed any eye problems up to this point. Pt has had normal development. • PMH, PSH, FHx – negative • Birth Hx – normal pregnancy and birth without complications
Case Presentation • VA sc OD 20/400 OS 20/20 • Stereo Vision 0/3 Animals, 0/9 Circles • Motility Full OU • OrthoTropic and OrthoPhoric • Bruckner sc brighter reflex OS • Pupils equal, round, reactive to light and accommodation; No APD OU
Case Presentation • PLE • Normal Facial Features • LLL WNL OU • Conj Clear and Quiet OU • Cornea Clear and Compact OU • A/C Deep and Quiet OU • Iris Normal OU • Lens Clear OU
Case Presentation Cyclopegic Retinoscopy • OD –3.25 +1.75 x85 • OS +1.00 +0.50 x93 • Fundoscopic Exam
Differential Diagnosis • Optic Nerve Coloboma • Morning Glory Anomaly • Peripapillary Staphyloma • Optic Disc Drusen • Megalopapilla • Optic Disc Dysplasia • Glaucomatous Cupping • Optic Pits
Differential Diagnosis – Syndromes • CHARGE • Coloboma, Heart defects, choanal Atresia, Retarded growth and development, Genital and Ear anomalies • Aicardi – death usually occurs in first few years of life • Multiple depigmented chorioretinal lacunae clustered around disc, congenital disc anomalies • Epileptic seizures, agenesis of corpus callosum, psychomotor retardation • Alagille • Posterior Embryotoxon and retinal pigmentary changes, eccentric pupils • Jaundice, heart defects, poor school performance
Differential Diagnosis – Syndromes • Edwards • Optic Atrophy, congenital glaucoma, corneal and lens opacities • Failure to thrive, heart defects, mental retardation • Lenz Microphthalmia • Coloboma, microcornea, microphthalmia • Severe renal dysgenesis, dental anomalies, severe speech impairment, short stature • Patau – fatal in first few months of life • Coloboma, microphthalmia, cataracts • Heart defects, cerebral hypoplasia, renal abnormalities, respiratory involvement, GI disease, urogenital involvement
Morning Glory Anomaly • Named after resemblance of optic nerve to the Morning Glory flower • Incidence is unknown, but very rare • Congenital abnormality • Sporadic, not inherited – colobomas run in families • Usually unilateral – colobomas bilateral • More common in females – equal in coloboma and staphyloma
Morning Glory Anomaly • Pathogenesis unknown • Abnormal closure of embryonic fissure (like coloboma) • Abnormal development of distal optic stalk at its junction with the primitive optic vesicle • Disc enlarged with funnel-shaped excavation centrally – coloboma inferior temporal, staphyloma normal disc sunken and cup shaped • Central core of whitish glial tissue, either elevated or recessed, representing persistent hyaloid remnants - unique
Morning Glory Anomaly • Surrounding elevated annulus of chorioretinal pigmentary disturbance – not seen in colobomas • Increased number of blood vessels, difficult to distinguish arteries from veins, which emerge in radial pattern from disc like spokes on a wheel - unique • Unusual phenomenon of contractile movements of the optic disc due to cuff of smooth muscle tissue in terminal optic nerve
Morning Glory Anomaly • Visual potential from 20/20 to NLP, usually 20/100 to 20/200 • Serous retinal detachment develops in about 30% of patients • Systemic associations rare • Frontonasal dysplasia • Hypertelorism, depressed nasal bridge, hare lip, or cleft palate • Basal encephalocele, absent corpus callosum, or pituitary deficiency • Neurofibromatosis type 2
Work-up, Treatmentand Follow-up • CT or MRI Head for possible Basal Encephalocele • Referral to pediatrician • Given full glasses prescription • Trial of patching, but should be discontinued if no improvement • Regular follow-up for retinal detachment • Spontaneous reattachment has been reported • Haik, et al. Ophthalmology. 1984 Dec;91(12):1638-1647
Results • Obtained CT Head • normal orbits, symmetrical and normal optic nerves, no intracranial masses, fluid collections or cystic structures • Referred to pediatrician • Given Rx • OD -3.25 +1.75 x85 • OS plano +0.50 x93 • Patching OS 7 hours/day for 5 days/week • 5 weeks later VA cc OD 20/200 OS 20/20 • Follow up in 3 months
References • Kanski, JJ. Clinical Ophthalmology: A Systemic Approach. 5th ed. Elsevier Science Limited; Philadelphia. 2003. • Dutton, GN. Congenital disorders of the optic nerve: excavations and hypoplasia. Eye. 2004;18(11):1038-1048. • Pollock, S. The morning glory disc anomaly: contractile movement, classification, and embryogenesis. Doc Ophthalmol. 1987 Apr;65(4):439-60. • Roy, FH. Ocular Syndromes and Systemic Diseases. 3rd ed. Lippincott Williams and Wilkins; Philadelphia. 2002. • Simon, JW, et al. Pediatric Ophthalmology and Strabismus. AAO; San Francisco. 2005; 339. • Chan, RT, et all. Morning glory syndrome. Clin Exp Optom. 2002;85(6):383-388. • Pictures www.atlasophthalmology.com