Download

1 / 33
360 likes | 528 Vues
Learn about the importance of blood culture testing for diagnosing bacteremia and septicemia. Find out how to collect specimens properly and the sources of bacteremic spread for various infections. This guide provides detailed steps for blood collection and culturing techniques.

E N D
BLOOD CULTURE ATOSA DORUDINIA; MD; APCP
Blood culture Aim of the test • An etiological diagnosis of bacteremia by aerobic and anaerobic cultivation of the blood, with identification and susceptibility test of the isolated organism(s). • Blood culture should be made for cases with suspected septicemia, endocarditis, and bacteremia secondary to localized infections (pneumonia, intra abdominal abscesses, pyelonephritis, epiglottitis, meningitis). In this case the blood culture may provide an etiological diagnosis of the localized infection. Types of specimen • Whole blood.
Culture of blood is essential in identifying: • Bacteriema • Sepsis • Infections of native and prosthetic valves • Suppurative thrombophlebitis • Mycotic aneurysm • Infections of vascular grafts • Invasive or disseminated infections ( bacteria, fungi)
Source of bacteremic spread • Pericarditis: • Polymicrobial • Bacteroids/ clostridium/ S.pyogenes/staph.aureus • Peritonitis: • Staph epidermidis, aureus/ gram-negative bacteria
Source of bacteremic spread • Pneomonias: • S.aureus, pneumoniae, • Pseudomonas, • H.influenza, • enterobacter
Source of bacteremic spread • Pressure sore: • Polymicrobial • proteus mirabilis • S. aureus • Bacteroidesfragilis • Acinetobacter • Bacillus
Source of bacteremic spread • Prostetic devices: • Endogenous skin or gut flora • Total hip replacement: • In malignacies/ steroid therapy/ CVD/ alcoholism
Source of bacteremic spread • Skeletal muscle: • S.aureus/ pseudomonas • Skin & soft tissues: • S.aureus/ strep betahemolytic/ pseudomonas/bacteroids
Fever • Hypothermia • Leukocytosis • Granulocytopenia • Hypotention
SPECIMEN COLLECTION • Skin first cleaned by alcohol 70%, then iodonesulution (1-2%) • Wash with soap/ rinse/ (povidone) iodone solution/ alcohol • 1-2 min let to dry • Each set of BC with separate venipuncture • If necessary to draw a culture through an intravenous line , another blood culture should be collected simultaneously to aid in interpretation of contaminated line.
Collection of Blood for Culturing • During blood culture collection all percussion should be taken to minimize the percentage of contaminated blood culture, to reduce the chance of contaminating organisms from the skin the vein puncture site should ideally be prepared as follows; • Wash with soap, rinse with sterile water or saline. • Apply 1-2 % tincture of iodine or povidone –iodine and allow drying for 1-2 minutes. • Remove the iodine with 70 % alcohol wash, if the site again be palpated after the iodine – alcohol preparation the finger must be disinfected or sterile gloves worn. • A tourniquet is applied to the upper arm above the vein puncture site to distend the anticubital veins.
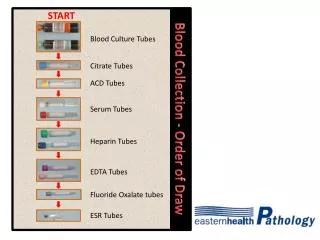
Collection of Blood for Culturing • Remove Flip Caps from the tops of the selected culture bottles. Disinfect the septa of the bottles with alcohol or iodine preparation and allow to dry. • Perform venipuncture with syringe and collect the desired amount of blood. If the vein is missed a new needle should be used. • Transfer the recommended amount of blood into the culture bottles using aseptic technique if desired. First fill the aerobic bottle. Do not overfill the bottles! Any remaining blood may be used for additional tests. • Label the bottles according to the routine procedure. When using a sticker do not cover the tear-off section of the barcode label . Note: 1:5 to 1:10 blood/broth ratio is the appropriate ratio to achieved, this dilution minimizes the effects of microbial inhibitors present in blood and dilutes any antimicrobial agents.
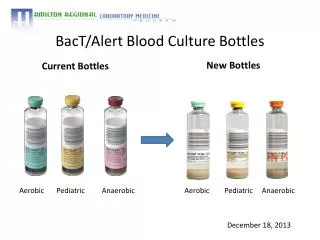
Blood bottles Trytic soy broth (TSB) Pancreatic digest of casien. Enzymatic soy digest. Sodium chloride. Dipotassium phosphate. Dextrose. Sodium polyanetholsulphonate(SPS) Fluid thioglychollate medium (FTM) Pancreatic digest of casien. Enzymatic soy digest. Sodium chloride. Dipotassium phosphate. Dextrose. Sodium polyanetholsulphonate(SPS) Sodium thioglychollate. agar.
Blood bottles A set of blood culture: one aerobic bottle and one anaerobic bottle.
Systems for processing BC • Manual • Lysis-centrifugation systems/ fastidiusbacterias • Automated and computerized systems
APPROPRIATE TIME • Before use of systemic antimicrobials • If therapy started cultures should still be obtained, if negative , must be interpreted with circumspection • Just before the chill ( not predictable)/ fever spike • Daily culture should not be condoned • Additional specimen after 3 days • Inoculated bottles immediately inverted • Transport to laboratory in room temperature • NEVER REFRIGRATED
Collection Time • Before starting antibiotics therapy if time permits, its generally recommended that the first two sets of blood cultures be taken one hour apart and the third set after 3-6 hours. • Obtaining the blood culture one half hour before a temperature spike is ideal because the highest concentration of organisms are circulating at that time, because the temperature spike is usually un predictable an educated guess must suffice in most cases when timing blood cultures.
SECIMEN VOLUME • Number of specimen collected is less important than the total volume of blood cultured • Adults: 20-30 ml/ culture set • Children: 1-5 ml/ culture set • Each set contains one aerobe and one anaerobe bottle, 10ml per bottle
SPECIMEN DRAWS • Two or three 20-ml blood sample/ 24 h • 30-60 min interval for the first two sets • If symptoms persists one or two sets in remaining 24 h • Urgent antibiotic therapy: separate sites within a few minutes
Frequent blood contaminants • Coagulase-negative Staph • Viridans strep • Bacillus other than B.anthracis • Corynebacterium • Propionobacterium • Two sets per friable episodes help distinguish pathogens from contaminants
CLINICALLY SIGNIFICANT ISOLATES • Gram negative bacili • Yeasts • Beta hemolytic sterptococci • Strep pneumoniae • Enterococci • Staph aureeus
Coagulase-negative staph problematic isolate Identification od isolate to the level of species Time to initial positivity Number of other negative sets Molecular typing Clinical data Antibiogram and identification of strain If both of are the same likelihood of true infection increases.
QUALITY ASSURANCE • LESS THAN 3% OF BCs SHOULD BE CONTAMINATED.
Specimen processing • The bottle incubated for 24 hour before plating to enhance the growth of bacteria, aerobic bottle plate on blood agar, MacConky, and chocolate in CO2 incubator for 24 hour, anaerobic incubate anaerobically on blood agar for 48 hour, and the negative bottle should be reincubated and tested after 10 days before discarded as negative culture. If slow growing organisms are suspected as Brucella spp. its should be clearly indicated on the requisition form and the culture bottles should be further incubated for 2-4 weeks before being reported out as negative.
POSITIVE CULTURES • Usually detected within 12-36 h • Initial report of Gram stain • After 24-48 h identification and susceptibility
SPECIAL CONFIGURATIONS • Fastidious organisms and endocarditis • Intravenous catheter cultures
Intravenous catheter cultures • Tip of catheter is rolled across the surface of an agar plate • >15 CFU associated with catheter-associated sepsis • Quantitative blood culture simultaneously through the catheter and by venipuncture • If cath is secondarily infected fewer CFUs through cath is obtained • If cath is the source the reverse will be obtained
How to culture an intravenous catheter tips • When colonization of an indwelling catheter is suspected of being the focus for septicemia, the catheter tip may be cutured to determine its status. • After overnight incubation the colonies are counted, A positive culture result with greater than 5 CFU.
Post specimen processing Interfering factors Patient on antibiotic therapy Result reporting Any isolated organism will be reported. Antibiotic sensitivity will also be included with the report. Turn around time Initial blood culture results will be reported as soon as it shows growth. Final results with sensitivity will be issued after 24- 48 hours of the initial report. Negative results will be issued after 10 days of culture submission.
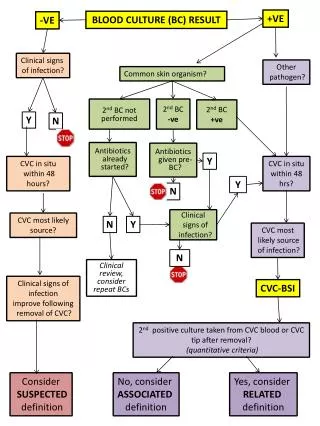
Interpretation of Positive Blood Cultures Virtually any organism, including normal flora, can cause bacteremia. A negative culture result does not necessarily rule out bacteremia; false-negative results occur when pathogens fail to grow. A positive culture result does not necessarily indicate bacteremia; false-positive results occur when contaminants grow. Gram-negative bacilli, anaerobes, and fungi should be considered pathogens until proven otherwise. The most difficult interpretation problem is to determine whether an organism that is usually considered normal skin flora is a true pathogen.