Download
1 / 1
10 likes | 162 Vues
A case of pneumatosis cystoides intestinalis attributed to an α- glucosidase inhibitor. Case: A 70-year old female Past history: Right knee osteoarthritis, autoimmune anemia (oral steroid administration), diabetes, angina Current history :

E N D
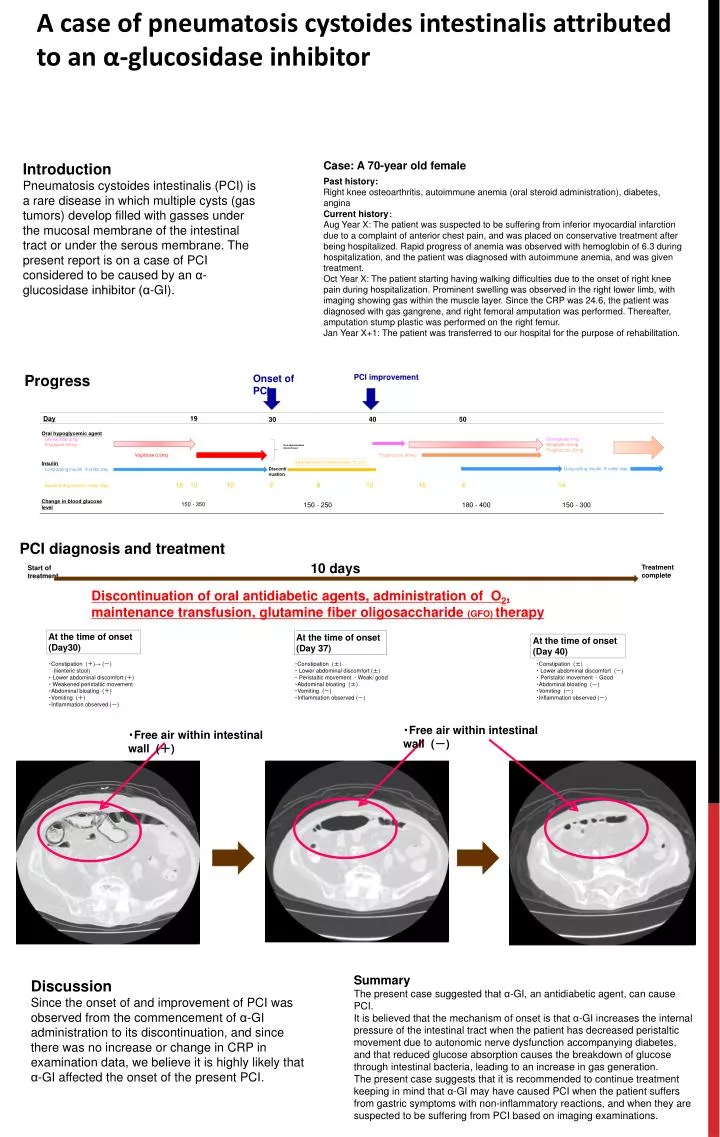
A case of pneumatosis cystoides intestinalis attributed to an α-glucosidaseinhibitor Case: A 70-year old female Past history: Right knee osteoarthritis, autoimmune anemia (oral steroid administration), diabetes, angina Current history: Aug Year X:The patient was suspected to be suffering from inferior myocardial infarction due to a complaint of anterior chest pain, and was placed on conservative treatment after being hospitalized. Rapid progress of anemia was observed with hemoglobin of 6.3 during hospitalization, and the patient was diagnosed with autoimmune anemia, and was given treatment. Oct Year X: The patient starting having walking difficulties due to the onset of right knee pain during hospitalization. Prominent swelling was observed in the right lower limb, with imaging showing gas within the muscle layer. Since the CRP was 24.6, the patient was diagnosed with gas gangrene, and right femoral amputation was performed. Thereafter, amputation stump plastic was performed on the right femur. Jan Year X+1: The patient was transferred to our hospital for the purpose of rehabilitation. Introduction Pneumatosis cystoides intestinalis (PCI) is a rare disease in which multiple cysts (gas tumors) develop filled with gasses under the mucosal membrane of the intestinal tract or under the serous membrane. The present report is on a case of PCI considered to be caused by an α-glucosidase inhibitor (α-GI). Progress PCI improvement Onset of PCI PCI diagnosis and treatment 10 days Treatment complete Start of treatment Discontinuation of oral antidiabetic agents, administration of O2, maintenance transfusion, glutamine fiber oligosaccharide (GFO) therapy 19 Day 50 40 30 At the time of onset(Day30) At the time of onset(Day 37) At the time of onset(Day 40) Glimepiride 1mg Sitagliptin 50mg Pioglitazone 30mg Oral hypoglycemic agent Glimepiride 2mg Sitagliptin 50mg Oral administration discontinued ・Constipation (+)→ (-) (lienteric stool) ・Lower abdominal discomfort (+) ・ Weakened peristaltic movement ・Abdominal bloating (+) ・Vomiting (+) ・Inflammation observed(-) ・Constipation (±) ・ Lower abdominal discomfort (±) ・Peristaltic movement - Weak/ good ・Abdominal bloating (±) ・Vomiting (-) ・Inflammation observed(-) ・Constipation (±) ・ Lower abdominal discomfort (-) ・Peristaltic movement - Good ・Abdominal bloating (-) ・Vomiting (-) ・Inflammation observed(-) Pioglitazone 30mg Voglibose 0.9mg Intra-transfusion insulin dosage21 unit Insulin Long-acting insulin4 units/ day Rapid-acting insulin( units/ day) Long-acting insulin8 units/ day Discontinuation 10 10 6 8 12 16 6 14 18 ・Free air within intestinal wall (-) ・Free air within intestinal wall (+) Change in blood glucose level 150- 250 180- 400 150- 300 150- 350 Summary The present case suggested that α-GI, an antidiabetic agent, can cause PCI. It is believed that the mechanism of onset is that α-GI increases the internal pressure of the intestinal tract when the patient has decreased peristaltic movement due to autonomic nerve dysfunction accompanying diabetes, and that reduced glucose absorption causes the breakdown of glucose through intestinal bacteria, leading to an increase in gas generation. The present case suggests that it is recommended to continue treatment keeping in mind that α-GI may have caused PCI when the patient suffers from gastric symptoms with non-inflammatory reactions, and when they are suspected to be suffering from PCI based on imaging examinations. Discussion Since the onset of and improvement of PCI was observed from the commencement of α-GI administration to its discontinuation, and since there was no increase or change in CRP in examination data, we believe it is highly likely that α-GI affected the onset of the present PCI.