Download
1 / 45
510 likes | 1.1k Vues
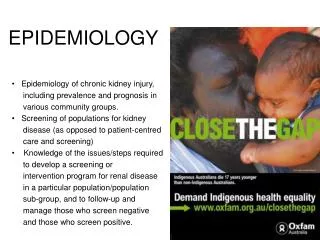
Hospital Epidemiology. What is it and what is it good for?. Edward O’Rourke , M.D Harvard University - Harvard Medical School. "It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm" Florence Nightingale .

E N D
Hospital Epidemiology What is it and what is it good for? Edward O’Rourke, M.D Harvard University - Harvard Medical School
"It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm" Florence Nightingale
Nosocomial infection =Any infection that is not present or incubating at the time the patient is admitted to the hospital
History of infection control and hospital epidemiology • Pre 1800: Early efforts at wound prophylaxis • 1800-1940: Nightingale, Semmelweis, Lister, Pasteur • 1940-1960: Antibiotic era begins, Staph. aureus nursery outbreaks, hygiene focus • 1960-1970’s: Documenting need for infection control programs, surveillance begins • 1980’s: focus on patient care practices, intensive care units, resistant organisms, HIV • 1990’s: Hospital Epidemiology = Infection control, quality improvement and economics • 2000’s: ??Healthcare system epidemiology modified from McGowan, SHEA/CDC/AHA training course
Why do we need hospital epidemiology?? Hospitals are complex institutions where patients go to have their health problem diagnosed and treated But, hospitals and medical/surgical interventions introduce risks that may harm a patient’s health
Consequences of Nosocomial Infections • Additional morbidity • Prolonged hospitalization • Long-term physical, developmental and neurological sequelae • Increased cost of hospitalization • Death
Challenges to the hospital epidemiologist • Make a hospital safe • Prevent harm to the patient and employees • initial focus on infectious diseases • increasingly all adverse (harmful) events are targets • Improve hospital efficiency • Eliminate unnecessary costs • Eliminate wasteful practices
What is hospital epidemiology? The fundamental roles of hospital epidemiology are to: • Identify risks • Understand risks • Eliminate or minimize risks
What is the role of hospital epidemiology? Identify risks to patient’s health • Find nosocomial infections • surveillance • Identify and study risk factors for nosocomial infection • understand epidemiologic principles and methods • case-control and cohort studies, bias, confounding • understand nosocomial pathogens • what is it about hospitalization that increases risk?
What is the role of hospital epidemiology? Eliminate or minimize risks to a patient’s health • organize care to minimize risk • eliminate risk factors • work around risk factors • develop improved policies and procedures • educate physicians and nurses regarding risks • study risk factors to learn more about them and how to eliminate them
Surveillance of nosocomial infections Outbreak investigation Develop written policies for isolation of patients Development of written policies to reduce risk from patient care practices Cooperation with occupational health Cooperation with quality improvement program Education of hospital staff on infection control Ongoing review of all aseptic, isolation and sanitation techniques Monitoring of antibiotic utilization Monitoring of antibiotic resistant organisms Eliminate wasteful or unnecessary practices Responsibilities of the Infection Control Program
Surveillance for nosocomial infection bloodstream infections pneumonia urinary tract infections surgical wound infections Patterns of transmission of nosocomial infections Outbreak investigation Isolation precautions Evaluation of exposures Employee health Disinfection and sterilization Hospital engineering and environment water supply air filtration Reviewing policies and procedures for patient care Areas of interest to a hospital epidemiologist
Antibiotic use Antibiotic resistant pathogens Microbiology support National regulations on infection control Infection control committee Quantitative methods in epidemiology Areas of interest to a hospital epidemiologist
Organizational topics in hospital epidemiology • Relationship of Hospital to External Agencies and Organizations • Personnel • Who does the hospital epidemiologist report to? • Authority • Resources
Authority of Infection Control Program • Accreditation mandates: Must meet for accreditation (example in USA: JCAHO) • Infection Control Program • Infection Control Committee • Authority statement • OSHA mandates: Safety regulations • Infection Control Department reports to Hospital Administration, not Medicine/Surgery or Nursing • Enhanced authority through cooperation, mutual respect, and shared goal of improving patient outcome
Regulatory approach External organizations establish rules and regulations Data collection for comparison with outside standards Inspections for compliance Penalties for non-compliance TQM/QI approach Internal organization of hospital staff to develop goals and methods Data collection for internal review Continuous efforts to improve Failure belongs to the entire system, not an individual QI versus Regulatory Strategies in Infection Control
Organizing for Infection Control • Requires cooperation, understanding and support of hospital administration and medical/surgical/nursing leadership • There is no simple formula: • Every hospital is different • Every hospital’s problems are different • Every hospital’s personnel are different • The hospital must develop its own unique program
Changes in Nosocomial Infection Rates in Hospitals with or without Effective Programs SENIC Study, CDC
Essential Components of an Effective Infection Control Program (after SENIC) • One full time infection control practitioner per 250 beds • optimal ratio may be different • A physician with training and expertise in infection control • Surveillance and feedback of rates to clinicians • Control activities (interventions, policies, training)
Personnel • Hospital Epidemiologist • MD with clinical training • Usually part time salaried by the hospital for infection control duties and part time as infectious diseases clinician • Training in infection control • Infection Control Practitioner • Usually a nurse but can be a microbiologist • Has clinical experience before entering infection control • Full time in infection control, no other clinical or administrative duties • Training in infection control
Organizing for Infection Control • Main elements • Develop an effective surveillance system • Establish policies and regulations to reduce risks • Develop with clinicians (physicians and nurses) • Develop and maintain a program of continuing education for hospital personnel • Use scientific (epidemiologic) method to study problems and test hypotheses
Organizing for Infection Control • Additional elements of an effective program • Antibiotic monitoring and control • Microbiologic laboratory liaison • Antibiotic susceptibility data dissemination • Occupational health • Provide resource to other departments for quality improvement study design and data analysis
Key elements of surveillance • Defining as precisely as possible the event to be surveyed (case definition) • Collecting the relevant data in a systematic, valid way • Consolidating the data into meaningful arrangements • Analyzing and interpreting the data • Using the information to bring about change adapted from R. Haley
Infection Control Committee Purpose • Advisory • Review ideas from infection control team • Review surveillance data • Expert resource • Help understand hospital systems and policies • Decision making • Review and approve policies and surveillance plans • Policies binding throughout hospital • Education • Help disseminate information and influence others
Infection Control Committee Committee Representatives • Hospital Epidemiologist • Infection Control Practitioners • Administrator • Ward, ICU and Operating room Nurses • Medicine/Surgery/Obstetrics/Pediatrics • Central Sterilization • Hospital Engineer • Microbiologist • Pharmacist
Qualifications to be on the committee Interest Represent group in hospital Experts in their field Diplomatic Good communicators Infection Control Committee
Resources: Where to get more information or help • Training Courses • Society of Hospital Epidemiologists of America (SHEA) • Association of Professionals in Infection Control (APIC) • National courses and congresses • Books • Textbooks: Bennett and Brachman - Wenzel - Mayhall • APIC Curriculum and Guidelines • CDC Guidelines • Journals • Infection Control and Hospital Epidemiology • Journal of Hospital Infections • American Journal of Infection Control • Consulting services • National: CDC, Ministry of Health • Colleagues
What is Hospital Epidemiology good for? • Infection control • Quality improvement • Controlling costs An effective hospital epidemiology program can help achieve all three goals
Risk factors for surgical wound infection • Age • Obesity • Malnutrition (low albumin) • Diabetes • Steroids/immunosuppression • Prolonged pre-op hospitalization • Infection at another site • Prolonged procedure • Drains • Urgency of surgery • Foreign body • Skill of surgeon
Strategies to develop effective patient care practices • Team collaboration • Staff education • Communication
Skin shaved the night before surgery Inappropriate peri-op antibiotic prophylaxis Instruments used for dressing changes submerged disinfectant Large containers of antiseptics, no routine for cleaning and refilling Eliminate shaving of skin the night before surgery Single dose peri-op antibiotic prophylaxis guidelines Use individual sterile packs of wound care instruments Use small containers of antiseptics; clean and dry containers before refilling Identify problems with polices and procedures Example: Pre- and Post-Operative Care Problem Area Recommendation
Methods to reduce cost of nosocomial infections • Reduce incidence • Reduce morbidity • Shorten hospital stay • Reduce costs of treating infections • Reduce costs of preventative measures • Stop ineffective control measures
Eliminate wasteExample: Unnecessary nursing techniques • Dressing change of aseptic wounds • Daily dressing change of venous catheter dressings • Daily change of intravenous infusion sets • Preoperative shaving • Routine changing of urinary catheters • Twice daily urinary catheter care • Protective gowns except for care of infected patients Daschner, F. J Hosp Infect (1991) 18, 73-78)
Eliminate waste:Unnecessary microbiologic monitoring • Routine environmental cultures of walls, floors, air, sinks, or other hospital surfaces • Routine cultures of healthcare workers nose and hands • Clinical cultures which are not available to clinicians in time to help with decision making Also: Failure to generate annual summary of culture data to provide clinicians with data for empirical selection of antibiotics
Cultures of Walls, Floors and Other Smooth Surfaces • All hospitals have some bacterial colonization of environment • What is the evidence that the environment directly infects the patient? • Hospitalized patients infect the environment • Poor technique, poor handwashing, poor disinfection have all been shown to infect the patients but these are all related to poor practice not the environment directly • Floors, Walls, Tables, Beds etc. should be cleaned properly but not cultured
Environmental Culturing: U. of Wisconsin Hospital Experience While maintaining standard hygiene and cleaning, degree of environmental contamination had no effect on infection rate
Prolongation of Hospital Stay due to Nosocomial Infections in the USA Adapted from Dixon, Ann Int Med 89:749, 1978
Annual Costs and Benefits of Infection Control Program in a Hypothetical 250-bed Hospital Each $1000 invested in infection control will return $3000 in net direct cost savings
Annual Nosocomial Infection Cost Savings by Introducing Effective Infection Control Program to a 250-bed Hospital
Antibiotic Prophylaxis in Surgery • Potentially an important part of surgical wound infection prevention • May also be a significant expense for the hospital • What is the cost-benefit of prophylactic antibiotics? • What is cost of wound infection? In money? In suffering? • How effective is prophylaxis? • How much can we spend to prevent a case of wound infection ?
Cost of Surgical Prophylaxis with Cefonocid in a Boston Teaching Hospital • Assuming $10 per course: • $178 to prevent one breast infection • $539 to prevent one herniorrhaphy infection • $1,515 to prevent one readmission for breast infection • $622 to prevent one readmission for herniorrhaphy From: Platt et al. NEJM 322:153, 1990.
Impact of Cefonocid Prophylaxis(per 1,000 patients) • Routine use for breast surgery would prevent • 56 infections • 23 definite wound infections • 16 UTIs • Routine use for herniorrhaphy would prevent: • 19 infections • 13 definite wound infections • from: Platt et al. NEJM. 322:153,1990.
Organization and support A. Institutional support • Infection control as a department • Placement in the organization • Authority • Personnel • Other resources
Organization and support B. Infection control committee • membership • support by the medical staff • participation by other disciplines • annual planning
Organization and support C. Infection Control Program • quality assessment • information for clinicians • educational/informational resource • surveillance data • outbreak investigation • assurance of appropriate asepsis, sterilization, disinfection • minimize risk from invasive procedures/devices • use of isolation • occupational health