Acute Otitis Media
Acute Otitis Media. Dr. Ghaleb Zughayar Consultant Pediatrician and Neonatologist. . Objectives Otitis Media. Demonstrate an understanding of pathophysiology List the common pathogens Demonstrate knowledge of both the advantages and disadvantages of antibiotic therapy

Acute Otitis Media
E N D
Presentation Transcript
Acute Otitis Media Dr. Ghaleb Zughayar Consultant Pediatrician and Neonatologist.
ObjectivesOtitis Media • Demonstrate an understanding of pathophysiology • List the common pathogens • Demonstrate knowledge of both the advantages and disadvantages of antibiotic therapy • Demonstrate application of an appropriate treatment plan
Definition • Acute Otitis Media (AOM) • “acute onset of symptoms, evidence of a middle ear effusion, and signs or symptoms of middle ear inflammation.” • Otitis Media with effusion (OME) • “Presence of MEE without signs or symptoms of infection, previously named: secretory, serous, or glue ear. ” Rudolph's Pediatrics - 21st ed 2002
Definition (continuous) • Difficult to treat AOM (20%) • Recurrent AOM: three or more episodes in the previous six months or four or more in the preceding twelve months. • Treatment failure AOM: a lack of improvement in sign and symptoms within 48-72 hours of AB treatment .
Definition (continuous). • Chronic Otitis media with effusion: OME that persists beyond three months. • CSOM: purulent otorrhea that persists for more than six weeks despite appropriate treatment for AOM.
Epidemiology • 31 million visits to physicians annually in U.S. • Most common diagnosis for an AB prescription in children. • Diagnosed > 5 million times a year. • 3-5 billion $/year in U.S. • 50,000 deaths / year worldwide. N Engl J Med 2002 347:1169-1174
Pathophysiology • Eustachian tube obstruction • Length: shorter in children • Angle: 10o children vs. 45o adult • Decreased immunocompetence • Follows upper respiratory infection (URI) • Peak incidence 2 - 4 days N Eng J Med 2002 347: 169-1174; Pediatr Infect Dis J 1996 15:281-291
Risk factors ● Age <2 years ● Atopy ● Bottle propping ● Chronic sinusitis ● Ciliary dysfunction ● Cleft palate and craniofacial anomalies ● Child care attendance ● Down syndrome and other genetic conditions ● First episode of AOM when younger than 6 months of age ● Immunocompromising conditions Pediatr Infect Dis J 1999 18:1-9
Specific Otalgia Otorrhea Dizziness Hearing loss Non-specific Fever (50%) Vomiting/diarrhea Anorexia Irritability Diagnosis: Clinical Manifestations
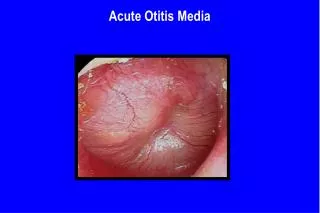
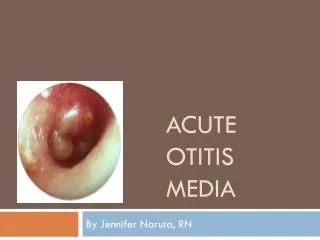
Diagnosis: Clinical Findings • Otoscopic findings • Bulging TM • Yellow, white, or bright red color • Opacification of eardrum • Impaired visibility of ossicular landmarks • Squamous exudate Rudolph’s Pediatrics - 21st ed 2002
Bacterial Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis Viral RSV Influenzae A & B Parainfluenzae 1,2, & 3 Rhinovirus Adenovirus Enterovirus Coronavirus Pathogens
Potential Complications • Hearing loss • Acute mastoiditis Rare: • Meningitis • Subdural/extradural abscess
Allergies AOM history Spectrum of activity Local resistance pattern Recent antibiotic treatment Age Duration Compliance Adverse drug events Cost Treatment Considerations
Treatment Considerations • Drug resistant S. pneumoniae (DRSP)incidence increasing • Patients at high risk for DRSP • Attending day care • < 2 years old • Antibiotic therapy in preceding 3 months
Why Focus on Pneumococcus? • Most common initial bacterial pathogen • Most common isolate after failed therapy • Least likely bacterial pathogen to self resolve • Most likely to cause severe otitis media • Most likely to cause suppurative complications of otitis (mastoiditis) Pediatr Infect Dis J 1998 17: 1084-1089
Treatment Options • AOM spontaneously resolves 40 - 60% • Symptomatic therapy • Applied heat, analgesics, antipyretics & topical anesthetic • Adjunctive therapy • Decongestants, antihistamines, & corticosteroids • Who to treat with antibiotics? • < 2 yo • AOM s/sx 3 days • Ill-appearing patients • Patients at an increased risk of DRSP N Engl J Med 2002 347: 1169-1174
Judicious Antibiotic Use • Proper diagnosis of AOM or OME before committing to antibiotic therapy • Diagnosis of AOM requires evidence of local inflammation & systemic symptoms • Erythema alone is not sufficient • Thickened, bulging and opaque TM • Pain • OME does not need immediate antibiotic therapy • Commonly seen with acute URI • Little or no benefit of antibiotic therapy • Persistent effusion expected for 2-3 months following therapy for AOM, but if persists > 3 months consider re-treatment
Amoxicillin: 1st Line Rationale Pediatric Infect Dis J 1999; 18:1-9 Pediatric Infect Dis J 1998; 17:1058-1059
How Effective is HD (90 mg/kg/d) Amoxicillin* Against Pneumococcus? Dagan et al. Poster 107, ICAAC 2000 *Study done w/ amox/clav but clav has no activity against pneumococcus
Treatment Failure • No improvement in ear pain, fever, or tympanic membrane otorrhea, bulging or redness after 3 days of antibiotic therapy • 2nd Line Therapy • DRSP • Beta-lactamase producing H.influenza and M. cattarhalis Pediatr Infect Dis J 1999 18:1-9
Prevention • Heptavalent pneumococcal conjugate vaccine (n=37,868) • Reduction of otitis office visits • Reduction of antibiotic prescriptions • Influenza vaccine • Goal: decrease number of URI • Breast feeding • Prophylaxis • 3 episodes in 6 months or 4 episodes in 1 yr • <6 months with >1 episode • Cause of resistance in the community Pediatr Infect Dis J 2003 22:10-16; Pediatr Infect Dis J 1998 17:1084-1089
In Summary . . . • Antibiotic resistance is here • High rates of antibiotic use in children has contributed to resistance rates • Vast majority of antibiotic use in children is for AOM • Minimizing unnecessary antibiotic prescribing can slow the rate of resistance • First line treatment of AOM is amoxicillin 90 mg/kg/day divided TID !!
DRSPBeta-lactam Activity & Levels Dowell SF et al. Pediatr Infect Dis J 1999 Apr; 18 (4): 341
Class Penicillin Considerations Most effective PO agent vs. DRSP Does NOT cover beta-lactamase producing H. flu or M.cat Tastes excellent Dosing SD: 40 mg/kg/day TID HD: 90 mg/kg/day TID (max 3 g/day) Adverse Events Rash Diarrhea Nausea/vomiting Contraindications Hypersensitivity to penicillins Dosage Forms Capsule Chewable Tab Tablet Suspension Amoxicillin
Augmentin®Selection after HD Amoxicillin Failure • Addition of clavulanate • No additional coverage for pneumococcus compared to amoxicillin • Augmentin ES® = 90 mg/kg/d of amoxicillin which is equivalent, NOT superior to HD amoxicillin for DRSP • Excellent coverage for beta lactamase positive H. flu and M. cat
Class Penicillin Considerations Equal DRSP coverage to amoxicillin Covers beta-lactamase producing H. flu & M.cat Food may enhance absorption, as well as decreases GI upset Tastes good Dosing HD 80 - 90 mg/kg/day TID (except XR)(max 3g/day amox) Adverse Events Nausea/vomiting Diarrhea Rash Contraindications Hypersensitivity to penicillins Dosage forms Suspension & chewable tablets 125/31.25/5 mL, 200/28.5/5 mL, 250/62.5/5 mL, 400/57/5 mL Susp ES 600 mg/42.9/5 mL Tablet 250 mg, 500 mg, 875 mg (125 mg clavulanate) Tablet XR 1000 mg/62.5 mg Amoxicillin/clavulanate(Augmentin®; Augmentin ES®; Augmentin XR®)
Oral Cephalosporins:Selection after HD Amoxicillin Failure All ORAL cephalosporins are LESS ACTIVE against DRSP than amoxicillin • No benefit for DRSP after failing high dose amoxicillin • Adds improved H. flu and M. cat coverage • Stable against beta-lactamase activity
Class Cephalosporin (2nd generation) Considerations Decreased efficacy against DRSP Efficacious against beta-lactamase producing H.flu & M.cat Requires food for absorption Tastes bad Dosing 30 mg/kg/day BID (max 1000 mg/day) Adverse Events Nausea/vomiting Diarrhea Rash Contraindications Hypersensitivity to cephalosporins Dosage forms Suspension Tablets Cefuroxime axetil
Class Cephalosporin (3rd generation) Considerations Decreased efficacy against DRSP Efficacious against beta-lactamase producing H.flu & M.cat Tolerable taste-banana/strawberry Dosing 14 mg/kg/day QD - BID (max 600 mg/day) Adverse Events Nausea/vomiting Diarrhea Rash Contraindications Hypersensitivity to cephalosporins Dosage forms Suspension Tablets Cefdinir
Ceftriaxone 3rd Generation Cephalosporin • Option when PO therapy fails • High middle ear fluid levels • Slightly better activity than amoxicillin • No comparison trial vs. HD amoxicillin for DRSP therapy • Requires 3 IM doses • 1 dose only has ~50% eradication of intermediate resistant strains of pneumococcus • 95% eradication of resistant strains • Little data on fully resistant DRSP (PCN MIC>2) Lebowitz E et al Pediatr Infect Dis 1998;17:1126
Class Cephalosporin (3rd generation) Considerations Good coverage against DRSP and beta- lactamase producing M. cat & H. flu Dosing 50 mg/kg QD for 3 days IM (max 1 gram) Adverse Events Nausea/vomiting Diarrhea Rash Contraindications Hypersensitivity to cephalosporins Dosage forms IM / IV Ceftriaxone
Non Beta-lactam Antibiotics Activity Against DRSP % Isolates Susceptible Pen-S Pen-I Pen-R Clindamycin 98% 90% 85% Erythromycin 96% 80% 51% Bactrim 94% 60% 20% Dowell SF et al. Pediatr Infect Dis J 1999
Clindamycin (Cleocin®)If HD Amoxicillin Failure • Excellent pneumococcal coverage • Active against 80-85% of DRSP strains • NO H. flu or M. cat coverage at all • Requires co-therapy with agent active against H flu (Bactrim, cefixime, etc.) • Palatability issue for suspension
Class Lincosamide Considerations NO coverage-H. flu or M. cat 15% cross resistance with DRSP Consider in combo tx for penicillin allergic patients Tastes awful Dosing 10 - 30 mg/kg/day TID (max 1800 mg/day) Adverse Events Nausea/vomiting Diarrhea Rash Increased LFT’s Contraindications Hypersensitivity to clindamycin Dosage forms Suspension Capsules Clindamycin: Cleocin®
MacrolidesIf HD Amoxicillin Failure Erythromycin – Azithromycin- Clarithromycin • 80% of penicillin intermediate and 50% of resistant strains remain fully susceptible to macrolides • H. influenza coverage generally less susceptible than with beta-lactams • All have good M. cattarhallis coverage
Class Macrolide Considerations DRSP ~ 50% cross resistance Decreased H. flu coverage Tastes okay - aftertaste Dosing 10 mg/kg x1 dose then 5 mg/kg QD for 4 days (max 500mg/250 mg) 10 mg/kg QD for 3 days (max 500 mg) 30 mg/kg x 1 (max 1500 mg) Adverse Events Nausea/vomiting Diarrhea Abdominal pain Rash Contraindications Hypersensitivity to macrolides Dosage forms Injection Suspension Tablet Azithromycin
Trimethoprim/Sulfamethoxazole(Bactrim®) • 20% of DRSP strains remain fully susceptible to Bactrim and significantly lower level of activity than with macrolides or clindamycin • H. influenza and M. cattarhallis coverage • Dosing: 6-12 mg/kg/day BID
Is it Rational to Treat AOM with Antibiotics to Prevent Mastoiditis? • Dutch strategy vs. US practice (100,000 children/year): • 2 additional mastoiditis cases in Netherlands • 7,800 more antibiotic prescriptions in US • 1,600 fewer adverse drug effects in Netherlands • # needed to treat = 3,900 to prevent 1 episode mastoiditis • Estimated antibiotic $ to prevent 1 episode = $117,000 (assumption $30/Rx) • 800 ADRs to prevent 1 episode mastoiditis • Additional cost to manage ADE? PIDJ 2001;20:140-4