Multiple Aneurysms
Multiple Aneurysms. Multiple Aneurysms. In 1982 Cohen et al reviewed 1500 patients with AAA 13% had multiple aneurysms 72% synchronously/28% metachronously Cause: 62% - nonspecific , 23% dissection Location: Abdominal – 63% Thoracoabdominal - 14% Descending aorta – 13%

Multiple Aneurysms
E N D
Presentation Transcript
Multiple Aneurysms • In 1982 Cohen et al reviewed 1500 patients with AAA • 13% had multiple aneurysms • 72% synchronously/28% metachronously • Cause: 62% - nonspecific , 23% dissection • Location: Abdominal – 63% Thoracoabdominal - 14% Descending aorta – 13% Aortic arch – 5% Ascending aorta - 5% Rutherford
Multiple Aneurysms • In 1990 Gloviczki et al reviewed 102 patients with multiple aneurysm – over two decades • Age: range 20 – 81 yrs • Total 201 aortic reconstructions – 3.4% of all aortic aneurysm performed during that time • Location: • Infrarenal – 30.9% • Descending aorta – 26.7% • Thoracoabdominal – 23.0% • Aortic arch – 19.3% JVS , 1990
Gloviczki et al, cont’d • 53.9% had Multiple aneurysm at first repair • 21 pts underwent simultaneous repair of at least 2 aortic aneuysm • 7 of the 21 pts (33.3%) died • 27 emergency procedures • 15 - rupture • 11 - pain • 1 – distal embolization with leg ischemia • 3 ruptured descending thoracic aneurysn • ( 4cm , 4 cm, 3.8 cm ) • One ruptured 2 days after AAA repair
Two stage operation for multiple aneurysms of the thoracic aorta,abdominal aorta and left common iliac artery in octagenarianKudaka et alJapanese Annal of Thoracic and Cardiovascular Surgery • AAA and iliac aneurysm resected first due to risk of thromboembolism 52 days later – Repair of descending aorta • Discharged home POD#25
Genetics and aneurysm • Familial clustering in 10-20% first degree relatives • Marfan’s (fibrillin ) • Ehler’s Danlos – type 4 ( procollagen III) • Aneurysms at an early age in these patients • Less type III collagen in aortic media • Abnormality on long arm of chromosome 16
Aneurysm Classification by Etiology Rutherford
Thoracoabdominal Aneurysms • Principle goal – prevent rupture and death • Most Surgeons choose to intervene when > 6cm • Smaller aneurysm followed by CT scan every 6 months • If expands > 5mm in 6 months – intervene • Patient with family history of AA • Women of small stature with 5cm aneurysm Cameron
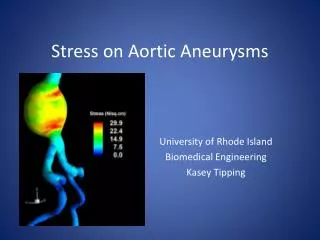
Spinal cord perfusion , minimize visceral organ ischemia and renal dysfunction
Visceral Aneurysms • Relatively uncommon • 25% present as emergency • 8.5% result in death • Frequency • Splenic – 60% F:M 4:1 , rupture during pregnancy • Hepatic – 20% M:F 2:1, trauma, IVD, inflammation • SMA – 5.5% Aggressive approach in management because of high mortality associated with rupture
Popliteal Aneurysm • Most frequent peripheral aneurysm – 70% • M:F 30:1 • >50% bilateral • 33% has AAA • Most common manifestation - thrombosis ( 40% ) - embolization ( 25% ) • 25% with distal thromboembolism come to amputation • Rupture – rare - < 5% Indication for treatment Acute lower limb ischemia from acute occlusion Transverse diameter > 2cm Sabiston