Download
1 / 53
560 likes | 985 Vues
Neurodegenerative diseases. Dr.HAZAR 2011. Neurodegenerative diseases. The main topics discussed are: mechanisms responsible for neuronal death, focusing on protein aggregation (e.g. amyloidosis), excitotoxicity, oxidative stress and apoptosis

E N D
Neurodegenerative diseases Dr.HAZAR 2011
Neurodegenerative diseases • The main topics discussed are: • mechanisms responsible for neuronal death, focusing on protein aggregation (e.g. amyloidosis), excitotoxicity, oxidative stress and apoptosis • pharmacological approaches to neuroprotection, based on the above mechanisms
pharmacological approaches to compensation for neuronal loss (applicable mainly to AD and PD).
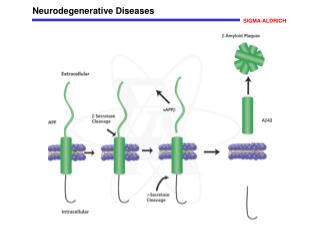
PROTEIN MISFOLDING AND AGGREGATION IN CHRONIC NEURODEGENERATIVE DISEASES • Many chronic neurodegenerative diseases involve the misfolding of normal or mutated forms of physiological proteins. Examples include Alzheimer's disease, Parkinson's disease, amyotrophic lateral sclerosis and many less common diseases. • Misfolded proteins are normally removed by intracellular degradation pathways, which may be altered in neurodegenerative disorders.
Misfolded proteins tend to aggregate, initially as soluble oligomers, later as large insoluble aggregates that accumulate intracellularly or extracellularly as microscopic deposits, which are stable and resistant to proteolysis.
Misfolded proteins often present hydrophobic surface residues that promote aggregation and association with membranes. • The mechanisms responsible for neuronal death are unclear, but there is evidence that both the soluble aggregates and the microscopic deposits may be neurotoxic.
Excitotoxicity and oxidative stress • Excitatory amino acids (e.g. glutamate) can cause neuronal death. • Excitotoxicity is associated mainly with activation of NMDA receptors, but other types of excitatory amino acid receptors also contribute. • Excitotoxicity results from a sustained rise in intracellular Ca2+ concentration (Ca2+ overload).
Excitotoxicity can occur under pathological conditions (e.g. cerebral ischaemia, epilepsy) in which excessive glutamate release occurs. It can also occur when chemicals such as kainic acid are administered. Raised intracellular Ca2+ causes cell death by various mechanisms, including activation of proteases, formation of free radicals, and lipid peroxidation. Formation of nitric oxide and arachidonic acid are also involved
Various mechanisms act normally to protect neurons against excitotoxicity, the main ones being Ca2+ transport systems, mitochondrial function and the production of free radical scavengers. • Oxidative stress refers to conditions (e.g. hypoxia) in which the protective mechanisms are compromised, reactive oxygen species accumulate, and neurons become more susceptible to excitotoxic damage
Excitotoxicity due to environmental chemicals may contribute to some neurodegenerative disorders. • Measures designed to reduce excitotoxicity include the use of glutamate antagonists, calcium channel-blocking drugs and free radical scavengers; none are yet proven for clinical use.
2011Memory and learning-1 Dr.HAZAR
Types of memory • There is general agreement that there are several different types of memory, each of which is predominantly in a different part of the brain.
Declarative vs. procedural memory • Declarative memory (explicit memory): • facts • dates • events • Hippocampus is critical • Procedural memory (non-declarative/implicit): • how to perform an act (ride a bicycle) • basal ganglia (dorsal striatum / caudate-putamen) is critical
Alzheimer' • Patients with Alzheimer's disease are unable to learn or remember ordinary facts (declarative memory) but are normal or nearly normal at learning and remembering how to do things (procedural memory).
Memory and the hippocampus • In 1950, a young man, known now by his initials, H.M. underwent brain surgery in Hartford, Connecticut. • H.M. was one of several patients in whom parts of the temporal lobe were removed in an effort to control epilepsy.
The temporal lobe is one of the four major divisions (lobes) of the brain, and is often the place in the brain attacked by epilepsy. • In H.M’s case, temporal lobe areas were removed on both sides of his brain. • After the surgery, his epilepsy was better, but he no longer had the ability to acquire new memories.
H.M became probably the most famous case in neurological history, and has been the subject of many studies. • Much of the initial work was carried out by Brenda Milner and her colleagues in Montreal.
Milner found that, although H.M could recall many of the events of his earlier life, he was unable to form new memories for experiences that occurred after the surgery. • He could remember things for a few seconds (short-term memories) but he couldn’t convert this information into long-term memories.
Analysis of H.M.’s lesion, based on the surgical report, indicated that the main temporal lobe areas affected were the hippocampus, amygdala, and parts of the surrounding cortex. • By comparing H.M.’s lesion with those in other patients, it seemed that the hippocampus was the area damaged most consistently in memory deficits.
At first, it was thought that H.M. had lost all ability to acquire new memories. • However, it was found that he could learn certain tasks.
Much is now known about the hippocampus, but we will mention just a few points. • Information about the external world comes into the brain through sensory systems that relay signals to the cortex, where sensory representations of objects and events are created
Outputs of each of the cortical sensory systems converge in parahippocampal region (also known as the rhinal cortical areas) which surrounds the hippocampus. • The parahippocampal region integrates information from the different sensory modalities before sending it to the hippocampus proper.
The hippocampus and parahippocampal region make up what is now called the medial temporal lobe memory system, which is involved in explicit or declarative memory.
The connections between the hippocampus and the neocortex are all more or less reciprocal • The pathways that take information from the neocortex to the rhinal areas and then into the hippocampus are mirrored by pathways going in the opposite direction. • Cortical areas involved in processing a stimulus can thereby also participate in the long-term storage of memories of that stimulus.
The rhinal areas serves as convergence zones, brain regions that integrate information across sensory modalities and create representations that are independent of the original modailty. • As a result, sights, sounds, and smells can be put together in the form of a global memory of a situation.
Many researchers believe that explicit memories are stored in the cortical systems that were involved in the initial processing of the stimulus, and that the hippocampus is needed to direct the storage process.
Early experiments on drug effects on memory • Certain post-training treatments can modulate memory storage in ways that enhance or prevent retention. • First observed with stimulant drugs • strychnine (very low doses) • amphetamine • caffeine
Early studies showed that drugs that inhibit protein synthesis also inhibit long-term memory formation. • Several inhibitors of RNA synthesis or protein synthesis block long-term memory, but do not affect short-term memory.
Gene transcription, translation, and memory • DNA is transcribed to produce RNA • RNA is translated to produce protein • DNA -> RNA -> protein • Transcription factors are proteins that regulate what genes are transcribed (expressed). • Transcription factors typically bind near the promoter region of a gene (the on/off switch).
How drugs act on synapses • Neurons communicate with each other at synapses using chemical neurotransmitters. • This provides the bases for drugs (and poisons) to affect synaptic transmission. • Drugs with chemical properties similar in some way to those of neurotransmitters can act on synapses to alter behavior and thoughts (psychotropic or psychoactive drugs)
Drugs that increase synaptic transmission are "agonists". • Drugs that block or reduce synaptic transmission are "antagonists".
About 25 neurotransmitters are known in the mammalian brain. • Most psychoactive drugs act on the synapses of a single neurotransmitter. • These synapses often occur in different, functionally unrelated parts of the brain, controlling many different behaviors • The psychological actions of drugs can be quite complex and difficult to predict
To affect the brain, drugs must cross the blood-brain barrier • Access to the brain from the circulatory system is controlled by the blood-brain barrier (BBB). • This barrier is made up of a layer of cell surrounding the blood vessels that supply the brain. • These cells determine the degree to which substances in the blood can enter the brain.
Fat-soluble substances (e.g., alcohol) cross the BBB more easily than water –soluble substances. • Drugs and hormones with large molecular weights do not easily pass the BBB. • Some substances, including glucose and insulin, are actively transported into the brain. • The degree to which drugs cross the BBB is critical to their effects on memory.
Loss of intellectual ability with age is considered to be a normal process, rate and extent of which is very variable
. Alzheimer's disease (AD) was originally defined as presenile dementia, but it now appears that the same pathology underlies the dementia irrespective of the age of onset. AD refers to dementia that does not have an antecedent cause, such as stroke, brain trauma or alcohol. Its prevalence rises sharply with age, from about 5% at 65 to 90% or more at 95.
Until recently, age-related dementia was considered to result from the steady loss of neurons that normally goes on throughout life, possibly accelerated by a failing blood supply associated with atherosclerosis. Studies since the mid-1980s have, however, revealed specific genetic and molecular mechanisms underlying AD (reviewed by Selkoe, 1993, 1997), which have opened new therapeutic opportunities
PATHOGENESIS AD is associated with brain shrinkage, and localised loss of neurons, mainly in the hippocampus and basal forebrain. Two microscopic features are characteristic : 1. Extracellular amyloid plaques, consisting of amorphous extracellular deposits of β-amyloid protein (known as Aβ), 2. Intraneuronal neurofibrillary tangles, comprising filaments of a phosphorylated form of a microtuble-associated protein (Tau). These appear also in normal brains, though in smaller numbers.
The early appearance of amyloid deposits presages the development of AD, though symptoms may not develop for many years. Altered processing of amyloid protein from its precursor (APP; see below) is now recognised as the key to the pathogenesis of AD. This conclusion is based on several lines of evidence, particularly the genetic analysis of certain, relatively rare, types of familial AD, in which mutations of the APP gene, or of other genes that control amyloid processing, have been discovered. The APP gene resides on chromosome 21, which is duplicated in Down's syndrome, in which early AD-like dementia occurs in association with overexpression of APP.
Loss of cholinergic neurons • Though changes in many transmitter systems have been observed, mainly from measurements on postmortem AD brain tissue, a relatively selective loss of cholinergic neurons in the basal forebrain nuclei is characteristic. This discovery, made in 1976, implied that pharmacological approaches to restoring cholinergic function might be feasible, leading to the use of cholinesterase inhibitors to treat AD .Choline acetyltransferase (CAT) activity in the cortex and hippocampus is reduced considerably (30-70%) in AD but not in other disorders such as depression or schizophrenia; acetylcholinesterase activity is also greatly reduced. Muscarinic receptor density, determined by binding studies, is not affected, but nicotinic receptors, particularly in the cortex, are reduced.
Cholinesterase inhibitors • Tacrine was the first drug approved for treating AD, on the basis that enhancement of cholinergic transmission might compensate for the cholinergic deficit. • Tacrine is far from ideal; it has to be given four times daily and produces cholinergic side-effects, such as nausea and abdominal cramps, as well as hepatotoxicity in some patients. Later compounds, which have limited efficacy but are more effective than tacrine in improving quality of life, include:
donepezil, which is not hepatotoxic • rivastigmine, a longer-lasting drug that is claimed to be CNS selective and, therefore, to produce fewer peripheral cholinergic side-effects • galanthamine, an alkaloid from plants of the snowdrop family, which is claimed to act partly by cholinesterase inhibition and partly by allosteric activation of brain nicotinic acetylcholine receptors