Download

1 / 13
140 likes | 264 Vues
A clinico-ethical framework for multidisciplinary review of medication in nursing homes. Wasim Baqir On behalf of the Shine Care . Edith. Unacceptable Patient Experience. Lack of structured review. Lack of patient involvement. Excess inappropriate medicines. Our objective.

E N D
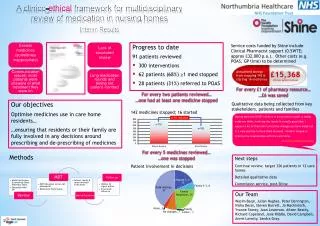
A clinico-ethical framework for multidisciplinary review of medication in nursing homes Wasim Baqir On behalf of the Shine Care
Unacceptable Patient Experience Lack of structured review Lack of patient involvement Excess inappropriate medicines
Our objective Optimise medicines use in care home residents… …ensuring that residents or their family are fully involved in any decisions around prescribing and stopping medicines
Key Learning • Not all patients have the capacity to make complex decisions • However, patients should have a say • Patient Involvement Framework • MDT Model • One size does not fit all, but… • Pharmacist, Care Home Nurse, Patient are key • GPs, POAS service
Key Results • 362 patients reviewed • 945 interventions • 54% (512) stop medicines in 219 patients (61%) • Start medicines, dose changes, dose forms, monitoring, etc. • Drugs stopped because • Unnecessary • Safety • Unwanted
Key Results • 362 patients reviewed • 945 interventions • 54% (512) stop medicines in 219 patients (61%) • Start medicines, dose changes, dose forms, monitoring, etc. • Drugs stopped because • Unnecessary • Safety • Unwanted • Financial Benefits • £55,000 saved on prescribing budget • Less nursing time to administer medicines • Reduced medicines waste
Involving Patients: our model 17% 40% 23% 4%
Family Perceptions “I think we should be notified if something was going to be stopped. [pharmacist] discussed about taking her off a Statin. But at the minute I think she is happy and has really good quality of life, I don’t think she should be taken off things without consulting the family with a good reason for her to be taken off them” “There is no point people being on things unnecessarily. You don’t need to be on them, why be on them”
What next? • Sustain • Business case to local CCGs • Local adoption by some practices • Adoption by neighbouring CCGs • Spread • Local marketing • National awards • Publication • Health Foundation
Our Team • Wasim Baqir – Project Lead • Annie Laverty (Director of Patient Experience) • Prof Julian Hughes (POAS/Newcastle University) – Clinical Lead • Nisha Desai/Steven Barrett – Clinical Pharmacists • Joanne Mackintosh – Patient Experience • Peter Derrington – Project Manager • Dr Jane Riddle – GP Advisor • Yvonne Storey – Communications • Richard Copeland – Head of Clinical Services • David Campbell – Chief Pharmacist • Sandra Gray (Director, Age UK) – Patient Advocate • John Connolly (Age UK) – Patient Advicate