Download
1 / 62
650 likes | 911 Vues
Learn how clinical biochemistry lab supports clinicians in diagnosing serous effusions efficiently. Understand types of effusions, classifications, differential diagnoses, fluid investigations, and special requests. Discover how biochemical tests help in differentiating transudates and exudates. Explore the significance of pleural fluid analysis in identifying underlying conditions.

E N D
Serous Effusions – how the clinical biochemistry lab can help the clinician Dr Damian Griffin Department of Clinical Biochemistry GUH
Shoot first, ask questions later! • Some biochemical investigations are only appropriate where specific rare diagnoses are considered • However, most of these investigations are very easy and inexpensive to perform • My policy is to do a full profile of potentially useful tests on all specimens, but avoid misleading tests
Effusions • A pathological extra-vascular collection of fluid in a body cavity or space • Pleural, peritoneal, pericardial, synovial • Ultrafiltrates with low protein concentrations and scant amounts of high molecular weight proteins reflect changes in permeability of filtering membranes • Fluids with high protein concentrations and significant amounts of large proteins such as immunoglobulins commonly result from infection or malignancy
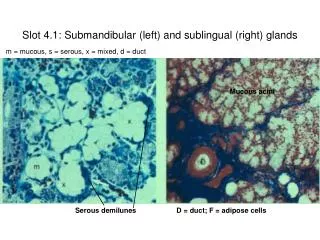
The pleura is a serous membrane which folds back onto itself to form a two-layered, membrane structure The thin space between the two pleural layers is known as the pleural cavity; it normally contains a small amount of pleural fluid. Pleura
The pleural cavity is a potential space lined by mesothelium of the visceral and parietal pleura It normally contains small amounts of fluid that facilitates movement of two membranes against one another This fluid is a filtrate derived from capillaries of the parietal pleura Produced at a rate dependent on capillary hydrostatic pressure, plasma oncotic pressure and capillary permeability Reabsorbed through the lymphatics and venules of the visceral pleura Pleural Fluid
A pathological accumulation of fluid in the pleural cavity, which results from an imbalance of fluid production and reabsorption Pleural Effusion
Transudate/Exudate Classification • Pleural effusions are commonly classified based on whether the pathology results in a transudate or an exudate • A pleural fluid protein conc. >35 g/L is consistent with an exudate • A pleural fluid protein conc. <25 g/L is consistent with a transudate. • If the protein conc. is 25-35 g/L, Light’s criteria are commonly used: • the pleural fluid is an exudate if one or more of the following criteria are met: • pleural fluid protein divided by serum protein >0.5 • pleural fluid LDH divided by serum LDH > 0.6 • pleural fluid LDH more than two-thirds the upper limits of normal serum LDH • In essence, this classification tries to differentiate pleural fluids resulting from imbalances in Starling’s forces from other causes
Transudates • Common • Cardiac failure • Hepatic cirrhosis • Hypoalbuminaemia (malnutrition, chronic disease, malabsorption) • Unusual • Hypothyroidism • Meig’s syndrome (ovarian fibroma associated with right pleural effusion) • Transudates are commonly bilateral
Exudates • Bacterial pneumonia • Tuberculosis • other granulomatous ds. e.g., sarcoidosis, histoplasmosis • Neoplasms • Brochogenic carcinoma • Matastatic carcinoma • Lymphoma • Mesothelioma • Non-infectious inflammatory disease • rheumatoid disease • systemic lupus erythematosus • Pulmonary infarct • Drugs • amiodarone, nitrofurantoin, phenytoin, methotrexate • Exudates are commonly unilateral
Fluid from extra-pleural sources • Pancreatitis • Ruptured oesophagus • Urinothorax • Chylothorax
Fluid Investigations • There are no further investigations on pleural fluid that will help with the differential diagnosis of a transudate • Gross examination • Microscopic examination • Chemical analysis • Microbiological examination
The Rogues Gallery Serous Blood-stained Anchovy sauce Milky
Microscopy • Malignancy can be diagnosed by cytology in 50-70% of cases • Evaluation of inflammatory cells numbers (neutrophils, lymphocytes or eosinophils) can aid the diagnosis • Immunocytochemistry can be helpful
Microbiology • Anaerobic & aerobic cultures • Culture for mycobacteria if TB suspected
Parapneumonic Effusions • Effusion that arises as a result of pneumonia, lung abscess or bronchiectasis • Up to 57% of pts with pneumonia develop effusion • Complications occur with bacterial invasion of damaged endothelium- neutrophil recruitment, activation of fibrinolytic system & fibrin deposition
Parapneumonic Effusions • Is commonly treated medically but may require surgical drainage if it is loculated or associated with a collection of pus (empyema) • Indications for surgical drainage include an effusion contains frank pus or where the pH <7.2
Trocar Catheter • This is why pH is important!
SPECIAL REQUESTS! • Amylase • Chylothorax • Urinothorax • Rheumatoid Arthritis
Amylase • Elevations above the serum level: • Oesophageal rupture (salivary isoenzyme) • Acute pancreatitis • Malignancy
Chylothorax/Pseudochylothorax • Disruption of the thoracic duct or its’ tributaries • Commonly malignancy (e.g. lymphoma) or trauma (e.g. surgery) • “Pseudochylothorax” – accumulation of cholesterol crystals in a long standing effusion • Triglyceride levels up to 4 times cholesterol level • Chylomicrons can be demonstrated by ultracentrifugation of after sitting specimen at 40C overnight
Urinothorax • Rare • 2o to obstructed kidney • Urine moves through peritoneum to cause effusion on the same side as the affected kidney • Smells like urine • Pleural fluid creatinine > serum creatinine • pH low
Rheumatoid Arthritis • Pleural involvement in 5% with RA • Fluid can be serous, turbid, yellow, green, milky or hemorrhagic • RA unlikely if fluid glucose is > 1.6 mmol/L • Glucose levels are not specific! • May be low in empyema, lupus, TB, malignancy and esophageal rupture • Elevated C4 complement levels (> 0.04 g/L) in pleural fluid is more specific
SUMMARY • Good clinical information needed • Macroscopic appearance • Apply Lights criteria if pleural fluid protein between 25 – 35 g/l • Pleural fluid pH should be performed in all non purulent effusions if infection is suspected • Special requests helpful in certain circumstances
Peritoneum • The peritoneum is the serous membrane that forms the lining of the abdominal cavity or the coelom • It covers most of the intra-abdominal (or coelomic) organs • It is composed of a continuous layer of mesothelium folded back on itself • The outer layer, the parietal peritoneum, is attached to the abdominal wall. • The inner layer, the visceral peritoneum, is wrapped around the internal organs that are located inside the intraperitoneal cavity • The potential space between these two layers is the peritoneal cavity filled with about 50 ml of serous fluid that allows the two layers to slide freely over each other
A pathological accumulation of fluid in the peritoneal cavity Ascites
Pathophysiology • In health a thin layer of peritoneal fluid, an ultrafiltrate of plasma, separates the two layers of peritoneum. • Ascites occurs when either fluid formation is increased or fluid removal is decreased. It is usually not apparent until more than 500 mL of fluid has accumulated. • Factors central to this include: • ↑ hydrostatic pressure gradient due to portal hypertension • ↓colloid osmotic pressure due to hypo-albuminaemia • ↑ permeability of the peritoneal capillaries • splanchnic arterial vasodilation • salt and water retention
Aetiology • Cirrhosis (80%) • Malignancy (10%) • Cardiac Failure (5%) • Tuberculosis
Fluid Protein • The transudate/exudate classification used in pleural effusions was not found to sub-divide the causes of ascites in a particularly useful way: • hepatic metastatic malignancy results in portal hypertension, a transudative process • the same cut-offs for transudate and exudate, largely because normal peritoneal fluid has a relatively high total protein • in practice exudative processes often give results in the transudative range and vice versa
Albumin Gradient • Serum ascites albumin gradient (SAAG) is defined as the serum albumin minus the ascitic fluid albumin concentration • It reflects the oncotic pressure gradient between the two compartments • A raised gradient (>=11 g/L) is associated with portal hypertension • provides a more useful classification system for ascites
Albumin Gradient • SAAG (>=11 g/L) • Malignancy – hepatic metastases (intrahepatic venous compression leading to portal hypertension • Cirrhosis • Congestive cardiac failure • SAAG (<11 g/L) • Malignancy – peritoneal (due to abnormal capillary permeability) • Tuberculosis • Pancreatitis • Nephrotic syndrome
Albumin Gradient Lab Concerns • Preanalytical factors are not normally considered • posture • prolonged tourniquet application • fluctuations in sick patients • diuretic use • Albumin methods are not validated for ascites • Dye binding methods • overestimate albumin at low concentrations • Bromocresol green methods are pH dependent • BCG methods are prone to interference from transferrin & lipoproteins. • Immunochemical methods are recommended but rarely used
Gross Appearance • clear straw coloured • cirrhosis • blood stained • clots on standing -> traumatic tap • homogenously blood-stained -> malignancy, pancreatitis, TB, intestinal infarction, abdominal trauma • chylous • due to lymphatic obstruction, e.g. malignancy • also • tea-coloured: pancreatic ascites • black: haemorrhagic pancreatitis or melanoma • dark molasses: perforated gut • green/brown: biliary tract disease
Non-biochemical tests • Cell count • spontaneous bacterial peritonitis (SBP) has a prevalence of 10-30% in ascites • >250 PMN/mm3 is diagnostic • indication for antibiotic therapy prior to culture • Bacterial culture • ascitic fluid should be inoculated into blood culture bottles immediately on sampling to improve sensitivity • Cytology • can detect peritoneal carcinomatosis
Biochemical tests that can add value • LDH • > 500 IU/L usually indicates malignancy, tuberculous or pancreatic ascites • Lower levels are less specific • Glucose • reflects the plasma concentration unless it is being metabolised by bacteria or fluid white blood cells • ↓ Glucose reported in TB peritonitis, carcinomatosis and SBP • early SBP glucose similar to that of sterile fluid • fluid:plasma glucose ratio < 0.7 is especially useful if considering TB peritonitis • Creatinine • helpful if asked is it urine • Bilirubin • >100μmol/L associated with biliary tract fistula or upper GI perforation
Biochemical tests that can add value • Fluid amylase • If the fluid amylase is greater than the serum amylase it suggests a pancreatic cause: • chronic pancreatitis • rupture of a pseudocyst • disruption of a pancreatic duct • ↑ amylase also in: • small bowel perforation/ischaemia • mesenteric thrombosis • lung or ovarian malignancy • Triglycerides • chylous effusions if >2.25 mmol/L • 80% associated with malignancy • Cholesterol • >1.8 mmol/L very good marker of peritoneal malignancy • not usually elevated with hepatocellular carcinoma
Biochemical Tests better avoided • Tumour markers • There is little added value to measuring traditional tumour markers in peritoneal fluid • Serum AFP is raised more commonly than peritoneal fluid AFP in proven hepatocellular carcinoma • Non-specific ↑CA-125, ↑ CA19-9, ↑ CA15-3 often found with endometriosis or pelvic pain • Adenosine deaminase • helpful in diagnosing tuberculous ascites • not readily available in most labs • pH • low values associated with SBP, but not until PMN count > 2000 • =>no added value
Pericardial Effusion • An abnormal accumulation of fluid in the pericardial cavity • Aetiology • transudative (congestive heart failure, myxoedema, nephrotic syndrome) • exudative (tuberculosis) • haemorrhagic (trauma, rupture of aneurysm, malignant effusion) • metastatic • Biochemical analysis has not been studied to a great extent
Pericardial Effusion • Cell Count & bacterial culture are useful • Exudate/Transudate • Light’s criteria has been validated in pericardial effusion • Glucose • <2.2 mmol/L common in bacterial, tuberculous, rheumatic or malignant effusions • pH • <7.10 may be found in rheumatic or purulent pericarditis • Triglycerides • chylous effusion • Post-mortem LDH, CK, troponin • in keeping with myocardial injury • ?TB • ADA & INF-γ largely superseded by PCR techniques • ?Lupus serositis • negative ANA makes diagnosis unlikely
Synovial Fluid • An ultrafiltrate of blood plasma combined with hyaluronic acid produced by the synovial cells • SF acts as a lubricant & adhesive and provides nutrients for the avascular articular cartilage • Laboratory examination is of major importance in differential diagnosis of joint disease, especially in crystal induced and infective arthropathies • Routine investigation is directed towards the diagnosis of these two disorders
Synovial Effusions Classification • Non-inflammatory • osteoarthritis, traumatic arthritis, neuropathic arthropathy, early rheumatic fever • early rheumatoid arthritis, early bacterial infections, viral arthritis • Inflammatory • rheumatoid arthritis, SLE, Reiter’s syndrome, acute crytal-induced arthritis, arthritis associated with inflammatory bowel disease, psoriatic arthritis, fat droplet synovitis • Purulent • bacterial, fungal, tuberculous • Haemorrhagic • traumatic arthritis, pigmented villonodular synovitis, synovial hemagioma, neuropathic osteoarthopathy, joint prostheses, and hematological disorders
Recommended Synovial Fluid Tests • Routine tests • Gross examination (colour, clarity) • Total & differential leukocyte counts • Gram’s stain and bacterial culture (aerobic & anaerobic) • crystal examination with polarizing microscope and compensator • Useful tests in certain circumstances • Fungal & acid fast stains and cultures • PCR for bacterial and mycobacterial DNA • Serum:synovial fluid glucose ratio • Lactate & other organic acids • Complement • Enzymes • Uric acid
Synovial FluidColour Straw common inflammatory or non-inflammatory causes Normal Red-Brown pathological haemarthrosis Brown septic Blood-stained trauma, diapedesis
Synovial FluidClarity • leukocytes are most commonly responsible for changes in clarity • shimmering oily appearance with cholesterol crystals