Mechanical Clot Detection
Mechanical Clot Detection . Stago’s Viscosity-based Clot Detection System. Viscosity based Detection System. Viscosity based Detection System. Viscosity based Detection System. Viscosity based Detection System. Viscosity based Detection System. NEW ANTICOAGULANTS. Katy Whelchel MT(ASCP)SH


Mechanical Clot Detection
E N D
Presentation Transcript
Mechanical Clot Detection Stago’s Viscosity-based Clot Detection System
NEW ANTICOAGULANTS Katy Whelchel MT(ASCP)SH Diagnostica Stago, Inc. Technical Support Specialist February 23, 2006
Maintain hemostatic balance • the body must maintain a fluid equilibrium • need to maintain balance between bleeding & clotting vessels “Coagulation” Proteins Platelets Fibrinolysis/ Inhibitors
ANTICOAGULANT THERAPY • Decrease the risk of post-op thrombosis • Decrease the risk of thrombosis in patients with risk factors • Decrease the risk of spontaneous abortions in patients with Anti-Phospholipid Syndrome (APS) - lupus anticoagulants
STANDARD ANTICOAGULANTS • HEPARIN (UFH) • COUMADIN (warfarin)
UFH – a few things to remember • Will affect PTT- how much depends dosing and your reagent system • Easily monitored (accurately!) with the Anti-Xa method • Can be used in patients with renal failure • HAS an antidote (protamine sulfate)
Coumadin –a few things to remember • Can be monitored by the PT/INR • Can be given long term for high risk patients • Can be used in patients with renal failure • HAS an antidote (Vitamin K)
2 classes of NEW ANTICOAGULANTS • Antithrombin Dependant • LMWH – Lovenox, Fragmin, Innohep (tinzaparin – has been used on CAP surveys) • DANAPROID (not available in US) • FONDAPARINUX (Arixstra) • Direct Thrombin Inhibitors • HIRUDEN – LEPIRUDEN (Refludan) • ARGATROBAN (Novastan) • Bivalirudin • Ximelagatran- the “new” coumadin
Why do we care about these new anticoagulants?? They are advertised as “no monitoring needed”!
Why do we care about these new anticoagulants?? • They can and DO interfere with our current coagulation tests • Can you say how much of this new drug is in the patient’s system? • What do you do for these patients? • Patient is bleeding • Patient is clotting – despite therapy • Pre-op assessment? • PT and PTT may or may not be “normal”
Why do we care about these new anticoagulants?? • Special patient populations need special consideration: • Pregnancy • Renal dysfunction • Liver dysfunction • Anorexic or morbidly obese patients
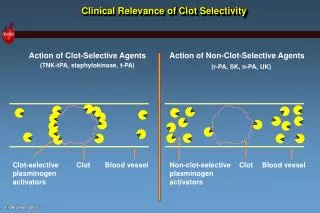
Heparins • UFH work on the activated factors • LMWHs work where the extrinsic and intrinsic factors come together with Factor Xa • Both use the patient’s ATIII to work
LMWH HEPARINS • LMWH – better bioavalibility than UFH • Created from UFH • Since it’s a smaller molecule it can be administered as a subcutaneous injection – given in fixed doses for MOST patients • Therapeutic Ranges: 0.5 – 1.1 (2 injections/day) 1.0 – 2.0 (1 injection/ day) • Timing of specimens - peak at about 4 hours after sub Q injection
LMWH HEPARIN • Doesn’t change the APTT (much) – an increased APTT may signify an overdose of LMWH or some other influence on the APTT (platelet antibodies) • Difficult to reverse with protamine sulfate (antidote for UFH) • Cleared through the kidneys
LMWH HEPARIN • LMWH available in the US: • Enoxaparin (Lovenox): prevent DVT/PE around surgery, treat DVT/PE, unstable angina • Dalteparin (Fragmin): prevent and treat DVT/PE, treat unstable angina • Tinzaparin(Innohep): treat DVT/PE
Who should be monitored for LMWH? • Patients with kidney problems (need to check creatinine clearance) • Patients that are obese or have a very low body weight • Children, burn patients
How should LMWH be monitored? • Monitor with an anti-Xa method, using LMWH calibrators and controls. • Samples should be drawn 4 hours after dosing.
DANAPROID (not available in the US) • Mixture of heparinoids • Usually given to HIT patients • Works through antithrombin to inhibit factor Xa (little effect on other factors) • Administered twice a day – IV or Sub Q • Therapeutic ranges – IV=0.5 – 0.8 Sub Q= 0.13-0.35 • Monitored by anti-Xa (like LMWH) – using danaproid as the calibrator.
Danaproid (cont’d) • It may prolong the PTT,as well as affect the PT, TT and ACT. • Used successfully in HIT – however, platelet count should be monitored. • No agent that will reverse the effects of the drug.
FONDAPARINUX (Arixtra) • Synthetic pentasaccharide – accelerates the binding of AT to Xa – the “ultimate LMWH” • Pure anti-Xa effect • Commonly used to prevent VTE in orthopedic surgery • Administered Sub Q • Half-life of 13 – 15 hours, so only 1 dose per day. • Excreted through kidney (check creatinine clearance…..)
Fondaparinux (cont’d) • PT and PTT are relatively insensitive to this drug, but may be slightly prolonged. • Low bleeding incidence. • Has not been shown to cause HIT • No direct inhibitor for Arixtra which can reverse it’s anticoagulant effect. • May be monitored by an Anti-Xa method using the drug as a calibrator.
Fondaparinux (cont’d) • Remember – there is no antidote. So if the patient has too much “on board”, the PT and PTT may be normal, but they may still be bleeding…….can use Factor VIIa concentrate (novoseven) or activated prothrombin concentrates to reverse effect.
DIRECT THROMBIN INHIBITORS • Hirudin – Lepirudin (Refludan) • Hirudin: Medicinal Leech • Refludan: recombinant polypeptide with same action • Agatroban • Bivalirudin (Angiomax) • Do not cause thrombocytopenia; used successfully with HIT • Directly blocks Thrombin • Administered by IV or Sub Q • REQUIRES MONITORING
DIRECT THROMBIN INHIBITORS • These drugs have a very short half life. • Agatroban cleared by the liver • Lepirudin is cleared by the kidneys. • Bivalirudin is cleared by the kidneys • Have to be aware of these factors with the patient!
ARGATROBAN • Derivative of amino acid arginine • Directly binds to Thrombin • Metabolized by the liver, and excreted through the kidney – so can be an alternate for patients with renal disease. • Must be monitored by APTT (can also be monitored by the ACT). Therapeutic range is 1.5-3.0 x Baseline APTT.
REFLUDAN - Lepirudin • APTT – IV=1.5 – 3.0 x patient baseline Sub Q= 2.2 – 2.7 X baseline APTT (specimen drawn 3 hours after administration) • HOWEVER, APTT reagents vary in their sensitivity to Refludin • ECARIN CLOTTING TIME (used in some facilities) • CHROMOGENIC ASSAY BASED ON THROMBIN INHIBITION (developed for research only at this point) – most accurate assay
DIRECT THROMBIN INHIBITORS • These drugs will affect the PT/INR – since they work at the bottom of the cascade • Lepirudin: recommend stopping drug once INR>2.0 • Agatroban: recommend stopping drug once INR>4.0 • Levels are PT reagent dependent!! Literature says that reagents with a lower ISI have less variability in reactivity. Higher ISI reagents have greater variablity in response. • Will affect results if patient is also on Coumadin!
DIRECT THROMBIN INHIBITORS • Since these drugs affect the PT/INR system – and since they have a very short half-life – the good news is that if they are discontinued for a couple of hours, the PT should return to normal. • The bad news is that the kidneys and liver have to be working for this to happen.
Bivalirudin • Approved for use in the cardiac cath lab • Bivalent thrombin inhibitor • Short half-life (20 -30 min) • Exclude patients with creatinine >3.0
DIRECT THROMBIN INHIBITORS • Ximelagatran – the “new Coumadin” • Oral tablet • Direct thrombin inhibitor • Converts to melagatran in the stomach • Cleared by kidneys • Irreversible – factor VII concentrate recommended for severe hemorrhage
DIRECT THROMBIN INHIBITORS Ximelagatran – the “new Coumadin” (cont’d) • it’s supposed to work better than our current LMWHs in preventing DVTs in people who have had hip surgery • Theoretically: NO MONITORING! It doesn’t matter how old you are, how much you weigh, etc. it is supposed to be safe…..however it causes liver damage in 6-10% of patients who take it long term. And remember – it is cleared by the kidneys.
DIRECT THROMBIN INHIBITORS Ximelagatran – the “new Coumadin” (cont’d) • Not approved by FDA – yet. • If you were going to monitor Ximelagatran, remember it is a thrombin inhibitor – so you’d have to monitor the APTT – NOT a PT even though it is the “new Coumadin”!! • APTT’s response again will be variable depending on reagent system.
DIRECT THROMBIN INHIBITORS Ximelagatran – the “new Coumadin” (cont’d) • So – for the time being, we’ll still be doing PT/INR for coumadin therapy.
Summary • Many of these anticoagulants are currently in use. • They may affect routine and specialty coagulation tests – remember where they affect the cascade! • If abnormal results are obtained, and not expected – ask what drugs the patient is on. • Remember many will act differently if the patient has renal or hepatic impairment. • The “tried and true” may still be the easiest to use if monitored correctly.