Female Genital Mutilation
290 likes | 667 Vues
Female Genital Mutilation. Dr Comfort Momoh FGM-Consultant/ Public Health Specialist. Masterclass. Safety and Quality Improvement Female Genital Mutilation. Setting the scene.

Female Genital Mutilation
E N D
Presentation Transcript
Female Genital Mutilation Dr Comfort Momoh FGM-Consultant/ Public Health Specialist
Masterclass • Safety and Quality Improvement • Female Genital Mutilation
Setting the scene • “I realised that my thighs has been pulled wide apart, and that each of my lower limbs were being held as far away from each other as possible, gripped by steel fingers that never relinquished their pressure. I felt that the rasping knife Or blade was heading straight down towards my throat.
Then suddenly, the sharp knife metallic edge seem to drop between my thighs and these, cut a piece of flesh from my body. I screamed with pain despite the tight hand held over my mouth, for the pain was not just a pain, it was like a searing flame through the whole of my body” (Davis A.Y.Women, Culture and Politics 1984)
FEMININE PAIN • And if I may speak of my wedding night: I had expected caresses. Sweet kisses Hugging and love. No Never • Awaiting me was pain. Suffering and sadness. • I lay in my wedding bed, groaning like a wounded animal, a victim of feminine pain.
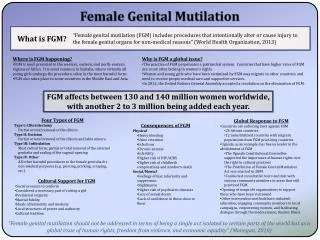
Gender Issues • FGM can sometimes be used by families as a powerful weapon to control the girl’s sexuality • As a means of deterring them from marrying outside their ethnic or religious communities • People believe that it is required by the religion
Geographical Area of FGM • Somalia 100% • Djibouti 100% • Sudan 90% • Ethiopia 90% • Burkina Faso 70% • Egypt 50% • Nigeria 50%
Why FGM • To safeguarded virginity • To control women's sexual power • To protect against rape or sexual activity of young girls • Uncircumcised women are seen as unclean, genital are seen as ugly • Uncircumcised women are believed to be infertile
Culture and Child protection • FGM is a very serious offence • It is dangerous to health • It is illegal in the UK • Penalty of 14years • It is an offence to take female child out of the UK for purpose or to arrange FGM
Role when aware a child is at risk of FGM • Referral to Social Services • Undertake preventative work via education to promote a better understanding of health and human rights implications of FGM • Provide as much information and support to women from practising communities to enable them to protect their daughters
Ensure that the message that is given out in respect of FGM is consistent across all health services • The aim must be to work in partnership with parents and families to protect children
FGM and the Law • Act 1985 • Act 2003 – changes: Penalty to 14years Extraterritoriality Name change
Health Professionals: Roles and Responsibilities • Protect and safeguard children • Be alert to the possibility of FGM • Be able to recognise FGM • Be able to act when a child is at risk or may already undergone FGM
Impact of FGM • Short term risk • Shock, Pain, Urinary Retention • Infection • Fracture or Dislocation • Injury to Adjacent tissue • Failure to Heal • Dermoid Cyst • Fistulae (Rectum or vaginal)
Intercollegiate Recommendation • Treat FGM as Child Abuse • Document and collect information on FGM and its associated complications in consistent and rigorous way • Share information on FGM systematically • Develop the competence, knowledge and awareness of a frontline professionals to ensure prevention and protection of girls at risk of FGM
Intercollegiate contd • Identify girls at risk and refer them as part of child safeguarding obligation • All girls and women presenting with FGM within the NHS must be considered as potential victims of crime, and should be referred to the police and support services
Intercollegiate contd • The NHS and local authorities should systematically measure the performance of frontline health professionals against agreed standards for addressing FGM and publish outcomes to monitor the progress of implementing these recommendations • Empowering and supporting affected girls and young women should be a priority consideration
Intercollegiate contd • Develop and implement national public health and legal awareness campaigns on FGM, similar to previous campaigns on domestic abuse and HIV
The African Well Woman’s Clinic • The clinic provides support, information and advice to women/girls who have undergone Female Genital Mutilation. We also provide a one stop clinic for surgical reversal of FGM. • For more information and referrals please call Comfort Momoh FGM Specialist on 02071886872 or 07956542576 or page her on 08700555500 (Code:881018) comfort.momoh@gstt.sthames.nhs.uk • Also provide training, conference and seminars for all professionals world-wide
Conclusion • As we know FGM is practised among migrant and refugee communities who tend to settle in urban areas. • The government policy of dispersing refugees and asylum seekers to rural, isolated centres has a major implications for women Who have experienced FGM.
Conclusion - contd • A better knowledge and understanding of the cultural factors relating to FGM is important in order to change people’s attitude. • It is vital that FGM laws are fully implemented and that governments, agencies, professionals and communities work together to end this practice.
Case 1 You are the G.P in a busy South London Surgery. A mother of two Somalian girls (aged 6 and 8) has come to you for some advice. She has recently been placed under a lot of pressure by her own family and in-laws to FGM her girls. She has been told that her daughters will not get married if they are not FGM and hence will bring shame on their family.
However, as she remembers how painful and violating the experience was, she does not want her children to go through the same experience. She asks you for advice
Question What would be your immediate response? What are the complexities of the situation? Who else is involved? How could you as clinicians combat the problem of FGM?
Case 2 You are the G.P in a busy South London Surgery. A 13 year old Ethiopian girl comes to the clinic with her mother, who is complaining that her daughter is ‘not herself’. You know the daughter well, and realise she is not her talkative, happy self. You ask her ‘what’s wrong’, and she replies; They’re going to cut me’
Question What would be your immediate response? What are the complexities of the situation? Who else is involved? How could you as clinicians combat the problem of FGM?
Case 3 You are the G.P. in a busy South London Surgery. As medicalisation is accepted in Egypt, the mother has approached you in the clinic, and has offered to privately pay you to conduct the FGM
Question What would be your immediate response? What are the complexities of the situation? Who else is involved? How could you as clinicians combat the problem of FGM?