
Trypanosomiasis: Hemoflagellates in Blood & Tissue
E N D
Presentation Transcript
Hemoflagellates in peripheral blood and tissue. Classified as 1. human tyrpanosomes- T cruzi, T brucei, T rangeli. 2. Animal trypanosomes- T. brucei brucei, T.evansi, T. lewisi, T. equiperdum.
T. cruzi • Causes South American trypanosomiasis or Chagas’ disease. • Amstigote form seen in RE cells. • Trypomastigote form seen in peripheral blood. • Disease mainly restricted to South and Central America.
MORPHOLOGY • Vertebrate host: two forms- amastigote and trypomastigote. • Insect host (reduviid bug): 4 forms- amastigote, promastigote, epimastigote, trypomastigote.
Host- 1. human 2. Insect(Reduviid bug) Infective form- Metacyclic trypomastigotes found in feces of the bug Mode of transmission- contamination of abraded skin, mucus membrane or conjunctiva become contaminated with feces of the bug containing infective form.
CLINICAL FEATURES • Incubation period- 1 week • Two types: Acute Chronic
Acute Chagas’ disease: characterised by 1. Chagoma 2.Romana’s sign 3. Generalized lymohadenopathy 4. Hepatospleenomegaly 5. Myocarditis and meningoencephalitis may be seen in children. Disease either resolves in 4-8 weeks or develops into chronic infection.
Chronic Chagas’ disease: Manifests years or decades after initial infection occurs due to multiplication of the parasite in the muscles - It can manifest as 1. Asymptomatic form 2. Cardiac form 3. Gastrointestinal form 4. Pulmonary form 5. Mixed form
Congenital trypanosomiasis: transmitted transplacentally I acute as well as chronic stage - Manifests as LBW, Still birth, Myocarditis or Neurological alterations In HIV infected patients there is greater risk of reactivation of underlying T.cruzi and they are more prone to develop meningoenceohalitis
LABORATORY DIAGNOSIS • Peripheral blood microscopy- detects trypomastigotes in acute stage. - Wet mount preparations - Thick and thin smears stained by Giemsa - Blood concentration techniques - Amastigotes demonstrated in heart tissues at autopsy.
Culture- Blood is inoculated on NNN medium, incubated at 25C and observed for30 days for presence of epimastigotes Antibody detection is useful in chronic and congenital infections Antigen detection can be done in urine and serum and is useful in diagnosing acute and congenital infection. Molecular methods Animal inoculation Xenodiagnosis
TREATMENT AND PROPHYLAXIS • Two drugs nifurtimox and benznidazole are available • The drugs are not much useful in chronic infections. • Prevention depends on vector control with use of insecticides, health education, housing improvement.
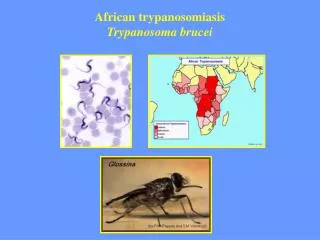
T.brucei • First demonstrated by Sir BRUCE • The complex consists of three subspecies T.brucei gambiense- chronic disease T.brucei rhodiense- acute and fatal disease T. brucei brucei- animal parasite
CLINICAL FEATURES • Stage I- systemic febrile illness due to dissemination of parasite through lymphatics and blood • Lymphadenopathy( winterbottoms sign) • Pruritus, maculopapular rash, • Delayed sensation to pain- Kerandel’s sign • Hepatospleenomegaly • Hematologic manifestations
Stage II disease: involves invasion to cns Invasion of perivascular areas alongwith infiltration of mononuclear cells Daytime somnolence, restlessness and insomnia at night Loss of spontaneity, abnormal speech, tremors CSF findings- increased CSF pressure, increased proteins, pleocytosis.
LABORATORY DIAGNOSIS • DIRECT MICROSCOPY • Blood examination:- • Specimen: Blood, Chancre fluid, CSF, Lymphnode aspirate. • Wet mount examination- highly motile trypomastigote. • Thick and Thin films • QBC capillary tube method
2. CSF examination - for Mott Cells- abnormal plasma cells. 3. Lymphnode aspirate – for T.brucei gambience. • ANTIBODIES FOR SERUM & CSF • Card agglutination test for Trypanosomes (CATT). • ELISA • Indirect Fluorescent antibody (IFA) test
ANTIGENS FROM SERUM AND CSF • ELISA • MOLECULAR METHODS • PCR • CULTURE • ANIMAL INOCULATION IN MICE
TREATMENT • Suramin and Pentamidine. • Eflornithine (alternate).