Download

1 / 128
1.28k likes | 1.42k Vues
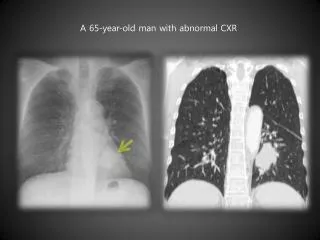
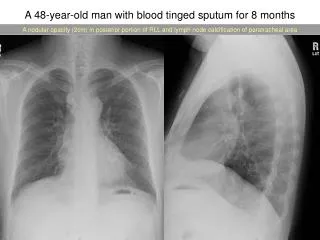
A 42-year-old asymptomatic man with hypertension presents for his annual physical examination. His medications include atenolol combined with chlorthalidone (at doses of 50 mg and 25 mg per day Both parents had type 2 diabetes mellitus later in life.

E N D
A 42-year-old asymptomatic man with hypertension presents for his annual physical examination. His medications include atenolol combined with chlorthalidone (at doses of 50 mg and 25 mg per day Both parents had type 2 diabetes mellitus later in life .
He does not smoke cigarettes. His body-mass index (BMI, the weight in kilograms divided by the square of the height in meters) is 32.3, and his blood pressure is 130/80 mm Hg . Would you screen the patient for diabetes, and if so, how?
American Diabetes Association Recommendations for the Screening of Asymptomatic Persons for Diabetes.*
Screen at any age and more frequently if the body-mass index is 25 or more and if the person has at least one additional risk factor
High-risk race (e.g., black, Native American, Asian, and Pacific Islander) or ethnic group (Hispanic
Glycated hemoglobin level of 5.7% or more or impaired fasting glucose or impaired glucose tolerance on previous testing
History of gestational diabetes or delivery of a baby weighing more than 9 lb (4.1 kg)
Hypertension (blood pressure ≥140/90 mm Hg; or therapy for hypertension
HDL cholesterol level of less than 35 mg per deciliter, triglyceride level of more than 250 mg per deciliter or both
Physical inactivity Other clinical conditions associated with insulin resistance (e.g., severe obesity and acanthosis nigricans
Age ↑ Family History / genetics ↑ Gestational Diabetes ↑ Obesity / fat distribution ↑ Physical Activity / fitness ↓ Smoking ↑ Very low birth weight ↑ Depression ↑ Antipsychotic medications ↑ Anti-Retrovial therapy ↑ Dietary Factors Carbohydratess ↓ Fats ↑↓ Glycemic load ↑ Cereal fiber / whole grain ↓ Dairy products ↓ High fructose corn syrup ↑ Sugar-sweetened bevarages ↑ Alcohol ↓ Coffee ↓ Summary: Risk Factors for Type 2 Diabetes
: AACE Diagnostic Criteria Glucose Testing and Interpretation
Criteria for the Diagnosis of Diabetes ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2.
Criteria for the Diagnosis of Diabetes *In the absence of unequivocal hyperglycemia, result should be confirmed by repeat testing. ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2.
Criteria for the Diagnosis of Diabetes *In the absence of unequivocal hyperglycemia, result should be confirmed by repeat testing. ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2.
Criteria for the Diagnosis of Diabetes ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2.
Criteria for the Diagnosis of Diabetes *In the absence of unequivocal hyperglycemia, result should be confirmed by repeat testing. ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2.
The diagnosis requires confirmation by the same or the other test.
Prediabetes: IFG, IGT, Increased A1C *For all three tests, risk is continuous, extending below the lower limit of a range and becoming disproportionately greater at higher ends of the range. ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 3.
AACE Recommendations for A1C Testing • A1C may be misleading in some clinical settings • Hemoglobinopathies • Iron deficiency • Hemolytic anemias • Thalassemias • Spherocytosis • Severe hepatic or renal disease • AACE/ACE endorse the use of only standardized, validated assays for A1C testing AACE. Endocrine Pract. 2010;16:155-156.
AACE Recommendations for A1C Testing • A1C should be considered an additional optional diagnostic criterion, not the primary criterion for diagnosis of diabetes • When feasible, AACE/ACE suggest using traditional glucose criteria for diagnosis of diabetes • A1C is not recommended for diagnosing type 1 diabetes • A1C is not recommended for diagnosing gestational diabetes AACE. Endocrine Pract. 2010;16:155-156.
, for every 25-32mg/dL in increase blood glucose levels, there is a 1% increase in HbA1c in patients But without any hematologic variants. 3 with patients who do have any hematologic disorders, this corresponding increase in HbA1c does not occur.
low values may occur in patients with certain hemoglobinopathies e.g., sickle cell disease and thalassemia) or who have increased red-cell turnover hemolytic anemiaand spherocytosis) or stage 4 or 5 chronic kidney disease, especially if the patient is receiving erythropoietin
In contrast, falsely high glycated hemoglobin levels have been reported in association with iron deficiency and other states of decreased red-cell turnover
Glycated hemoglobin Fasting not required, low biologic marker of long-term glycemia, stable during acute illness, sample stability in vial global, standardization, close association of results with complications variability,
A1C ~ “Average Glucose” A1C eAG % mg/dL mmol/L 6 126 7.0 6.5 140 7.8 7 154 8.6 7.5 169 9.4 8 183 10.1 8.5 197 10.9 9 212 11.8 9.5 226 12.6 10 240 13.4 Formula: 28.7 x A1C - 46.7 - eAG American Diabetes Association
A fasting glucose level of 100 to 125 mg is consistent with prediabetes; the range of glycated hemoglobin levels that are diagnostic of prediabetes is controversial, but the ADA recommends a range of 5.7 to 6.4%
Oral glucose-tolerance test Most sensitive test, earliest marker of glucose dysregulation
Fasting required, substantial biologic variability, poor reproducibility from day to day , lack of association of results with complications over time, sample instability in vial more time required, inconvenience,, higher cost, lack of global standardization of plasma glucose measurements
It disclosed wheathera subject has prediabetes • Test allowed established whether has an n GTTor unkown type 2 diabetes Approximately40%of subjects who will develo diabetes with the NGT OGTT detectsdiabetes more efficiently thanFBS
Sbject withFBS >100in GTT(60%)had 2hpg <140 • Subject withFBS <100 (14%)had 2hpg>.140
• Testing of glycated hemoglobin or fasting plasma glucose appears to identify different groups of patients with diabetes and prediabetes, yet both tests identify patients at similar risk for adverse sequelae.
Longitudinal investigations have shown that persons categorized as being “impaired” by any of these definitions have approximately a 5 to 10% annualized risk of diabetes, a risk that is greater by a factor of approximately 5 to 10 than that normal glucose tolerance or normal fasting glucose .
Risks appear to be similar among persons with isolated impaired fasting glucose (i.e., without impaired glucose tolerance) and isolated impaired glucose tolerance (without impaired fasting glucose). However, the proportion of patients with impaired glucose tolerance tends to be greater than that with impaired fasting glucose in most populations
Persons with both impaired fasting glucose and impaired glucose tolerance have a higher risk of diabetes (approximately 10 to 15% per year) than those with only one abnormality. Whereas both prediabetic states are associated with increased total and cardiovascular mortality, impaired glucose tolerance tends to be a better predictor than impaired fasting glucose.
Persons with both impaired fasting glucose and impaired glucose tolerance have a higher risk of diabetes (approximately 10 to 15% per year) than those with only one abnormality. Whereas both prediabetic states are associated with increased total and cardiovascular mortality, impaired glucose tolerance tends to be a better predictor than impaired fasting glucose.14
Type 2 Diabetes Screening in Children/Adolescents • Overweight -BMI >85th percentile -weight for height >85th percentile -weight >120% of ideal for height • Plus any two of the following risk factors….
Type 2 Diabetes Screening in Children/Adolescents • FH of type 2 diabetes in 1st or 2nd-degree relative • Race/ethnicity (Native American, African American, Latino, Asian American,Pacific Islander) • Signs of insulin resistance or conditions associated with insulin resistance (acanthosis nigricans, hypertension, dyslipidemia, PCOS, or small-for -gestational-age (SGA) birth weight) • Maternal history of diabetes or GDM during gestation Diabetes Care 34:Supplement 1, 2011
Type 2 Diabetes Screening for Children/Adolescents • Age of initiation: at-risk age 10 years or if younger onset puberty • Screen every 3 years • No screening recommended for Type 1 Diabetes in asymptomatic individuals outside of research protocols
Gestational Diabetes (GDM) • Screen for type 2 diabetes first prenatal visit if risk factors • Not known to have diabetes, screen for GDM at 24 –28 weeks of gestation • Screen women with GDM for persistent diabetes 6–12 weeks postpartum • Women with a history of GDM lifelong screening for diabetes or prediabetes at least every 3 years (up to 7x higher risk than non-GDM) Diabetes Care 34:Supplement 1, 2011Lancet, 2009, 373(9677): 1773-9 Diabetes Care 21(2):B161–B167, 1998 Diabetes Care 2010; 33: 676–682