Renal Pathology: Causes, Symptoms, and Treatment
Explore the complexities of acute and chronic renal failure, glomerulonephritis, and pyelonephritis. Understand the pathology, morphology, and histology of these conditions and learn about azotemia and uremia. Readings from Robbins Chapter 14.

Renal Pathology: Causes, Symptoms, and Treatment
E N D
Presentation Transcript
Aims • Renal Pathology • Acute renal failure • Chronic renal failure • Glomerulonephritis • Pyelonephritis • Readings: • Robbins; Chapter 14
Terms • Azotemia • Elevation of blood urea nitrogen (BUN) and creatinine levels largely related to a decreased GFR • Prerenal azotemia is encountered when there is hypoperfusion of the kidney. • Postrenal azotemia is seen when there is obstruction of urine flow below the level of the kidney. • Renal failure detectable only by lab tests • Uremia • Azotemia characterized by failure of renal excretory function in addition to metabolic and endocrine alterations resulting from renal damage. • Renal failure with clinical signs and symptoms
Acute Renal Failure • The kidney abruptly stops working entirely. • They can recover to normal function (____________________________________). • Acute glomerulonephritis • Acute tubular necrosis (ATN)
Acute Glomerulonephritis • Caused by abnormal immune reaction that damages the glomeruli. • Symptoms • Hematuria (blood in urine). • Oliguria (little urination). • Mild hypertension. • Proteinuria. • Edema.
Acute Glomerulonephritis • Onset • 95% of patients have bacterial infection 1-3 weeks before. • Usually group A beta streptococci.
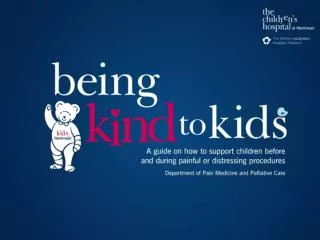
Acute Glomerulonephritis Morphology/ Histology • Enlarged hypercellular glomeruli. • Both leukocytes and mesangial cells. • “Humps” of antigen-antibody complexes. Robbins & Cotran’s Pathologic Basis of Disease 21-16
Acute Glomerulonephritis • Pathology • As antibodies build up, they bind antigen resulting in an insoluble immune complex which becomes entrapped in the _______between the endothelium and basement membraneorthe epithelium and the basement membrane Robbins Basic Pathology14-3
Acute Glomerulonephritis • Pathology • Antibodies against the endothelial basement membrane or the glomerular tissue bind to their target antigen and can block filtration or cause tissue injury in the long term (complement or phagocyte activation) Robbins Basic Pathology14-3
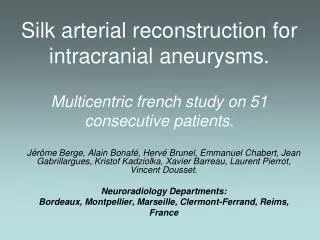
Acute Glomerulonephritis Histology • Circulating immune complexes accumulating in the glomerulus. • Granular fluorescent staining for immune complexes. • Immune complex forming in the tissue. • Linear fluorescent staining for immune complexes. Robbins Basic Pathology14-4
Acute Glomerulonephritis • Pathology • This results in proliferation of mesangial cells (cells between the endothelium and epithelium). • Entrapment of leukocytes in glomeruli. • Results in blockage of glomeruli. • Usually subsides in a couple of weeks. • Sometimes may lead to chronic renal failure.
Acute Tubular Necrosis (ATN) • Most common cause of acute renal failure. • Destruction of the epithelial cells in the renal tubules. • Ischemia • Poisoning • Toxins (ethylene glycol) • Medications (tetracyclines)
Acute Tubular Necrosis (ATN) • Pathology • Each of these causes results in the death of the renal tubular epithelium, which cause them to slough away from their basement membrane and plug up the tubules (casts). • If the basement membrane remains intact a new epithelium can grow repairing damage in 1-20 days.
Acute Tubular Necrosis (ATN) Morphology/ Histology • Ischemic ATN is characterized by focal tubular epithelial necrosis and apoptosis. • Rupture of basement membranes. Robbins & Cotran’s Pathologic Basis of Disease 21-35
Acute Tubular Necrosis (ATN) • Ischemic ATN • Occlusion of tubular lumens by casts of cell debris. • Especially vulnerable are the proximal tubule and the thick ascending limb. • _____________________. Robbins & Cotran’s Pathologic Basis of Disease 21-34
Acute Tubular Necrosis (ATN) • ATN due to poisoning most obviously effects the proximal tubule • Necrosis and occlusions. Robbins & Cotran’s Pathologic Basis of Disease 21-34
Chronic Renal Failure • Progressive loss of nephrons that gradually leads to kidney failure. • ______________________________________. • Chronic Glomerulonephritis • Chronic obstructive pyelonephritis
Chronic Renal Failure • Four stage process • Diminished renal reserve • GFR is ~50% of normal • Patients are asymptumatic. • Renal insufficiency • GFR is 20-50% of normal. • Symptoms include anemia, polyuria, and nocturia.
Chronic Renal Failure • Renal failure • GFR <20-25% of normal. • Kidneys can not regulate volume or solute concentration. • As a result patients develop edema, acidosis, and hypocalcemia. • Overt uremia (accumulation of urea, uric acid, and creatinine). • End-stage renal disease. • GFR is <5% of normal. • Loss of kidney function to the point at which the person must have a kidney transplant or dialysis treatment.
Chronic Glomerulonephritis • Inflammation and damage to the capillary loops in the glomeruli. • Onset • Slowly progressive. • Unlike acute glomerulonephritis not due to streptococcal infection.
Chronic Glomerulonephritis Morphology/ Histology In later stage disease there is obliteration of glomeruli transforming them into acellular eosinophilic masses. Robbins Basic Pathology14-13
Chronic Glomerulonephritis • Pathology • Begins with a precipitation of antigen-antibody complexes. • Result in inflammation and thickening of the membranes. • Ultimately leading to fibrosis of the glomeruli. • In the late stages the glomerular capillary filtration coefficient ____________________________________. • Decreased number of filtering capillaries. • Thickening of the membrane. • Can lead to nephrotic syndrome (increased plasma protein permeability in the glomeruli resulting in excretion of protein in the urine).
Chronic Obstructive Pyelonephritis • Injury to the renal interstitial tissue due to a bacterial infection (Acute pyelonephritis). • Infection usually derived from bacteria that has traveled from the bladder. • Urinary Tract Infection • Recurrent infections superimpose on one another. • Obstruction predisposes kidney to additional infections. • Symptoms • Back pain • Fever • Pyuria • Dysuria
Chronic Obstructive Pyelonephritis • Onset • Most commonly caused by E. coli infection originating from fecal contamination of the urinary tract (_________________________________ ).
Chronic Obstructive Pyelonephritis • Pathology • Begins in the _____________________________________. • Leads to scarring and abnormal nephron function.
Chronic Obstructive Pyelonephritis Robbins Basic Pathology14-14
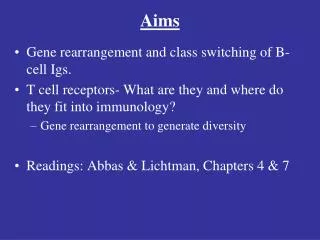
Chronic Obstructive Pyelonephritis Morphology Kidneys are irregularly scarred. Can vary from one to several in number. Most are in the upper or lower poles. Robbins & Cotran’s Pathologic Basis of Disease 21-43 & Robbins Basic Pathology14-16
Chronic Obstructive Pyelonephritis Morphology/ Histology Tubules show atrophy in some areas and hypertrophy in others. Dilated tubules can be filled with colloid casts. -Gives a thyroid gland appearance. Robbins & Cotran’s Pathologic Basis of Disease 21-43
Abnormal Nephron Function • Loss of water and electrolyte balance • Loss of functional nephrons requires the surviving nephrons to excrete more water and solutes. • Maintained until as much as 70% of nephrons are lost.
Abnormal Nephron Function • Decreased waste product excretion (urea and creatinine) • Begin to accumulate in serum as nephrons are lost. • Kidneys compensate by increasing the GFR and rate of flow through the remaining functional nephrons. • This can result in isosthenuria (inability to concentrate or dilute urine). Guyton’s Textbook of Medical Physiology 31-6
Abnormal Nephron Function • Uremia • Generalized edema • Acidosis • Each day the body normally produces 50-80 millimoles more metabolic acid than base. • High concentrations of urea and creatinine. • High concentrations of phosphates and potassium.
Abnormal Nephron Function • Anemia • Decreased secretion of __________________________________.
Abnormal Nephron Function • Osteomalacia • Weakened bones due to absorption of Ca++ & PO4-. • Decreased production of 1, 25 OH-Vitamin D. • Elevated plasma PO4- levels due to decreased GFR. • PO4- binds to Ca++ in plasma, stimulating PTH secretion and secondary hyperparathyroidism. Robbins Basic Pathology8-19
Kidney (Hemodialysis) Dialysis • Blood filtration to remove unwanted substances. • <500ml of blood at a time in the artificial kidney. • Heparin is added to prevent clotting. • 3 times a week for 4-6 hours. Guyton’s Textbook of Medical Physiology31-8
Kidney (Hemodialysis) Dialysis • No phosphate, urea, urate, sulfate, or creatinine in the dialyzing fluid. Guyton’s Textbook of Medical Physiology table31-7
Next Time • Prostate pathologies • Endometriosis • Toxemia of Pregnancy • Readings; Robbins, Chapters 18 & 19
Objectives • Describe the histology/morphology & pathology of acute renal failure. • Acute Glomerulonephritis & Acute Tubular Necrosis • Describe the histology/morphology, pathology & 4 stages of chronic renal failure. • Chronic Glomerulonephritis & Chronic Obstructive Pyelonephritis • Describe the results of abnormal nephron function. • Water and electrolyte balance, waste excretion, uremia, anemia, and osteomalacia • Describe kidney dialysis.