Download
1 / 27
270 likes | 524 Vues
CPR: Duration and Outcome. Jack P Freer, MD Professor of Clinical Medicine Daniel J Miori MS, RPA-C Palliative and Ethics Millard Fillmore Gates Daniel Sleve, M4. CPR. Unique —high stakes, life or death, stark Abrupt —must be refused in advance Standardized —routine, ACLS protocol

E N D
CPR: Duration and Outcome Jack P Freer, MD Professor of Clinical Medicine Daniel J Miori MS, RPA-C Palliative and Ethics Millard Fillmore Gates Daniel Sleve, M4
CPR • Unique—high stakes, life or death, stark • Abrupt—must be refused in advance • Standardized—routine, ACLS protocol • Universal—potential use: everyone • Iconic—represents promise and misuse of modern technical medical capabilities
CPR Decision Making • Presumption to treat • No decision=consent to CPR • Documentation regulated
Reasons to Use CPR • Benefits > Burdens • It’s good to be alive! • Burdens trivial by comparison • Desperation
Reasons to Refuse CPR(consent to DNR) • Little empirical data in literature • Theoretical construct • Tomlinson T. Brody H. Ethics and Communication in Do-Not-Resuscitate Orders.NEJM(1988) 318:43-6 • NYS DNR Law • Symbolism • Cynical view
Reasons to Refuse CPRTomlinson & Brody • No Medical Benefit—Futile • Poor Quality of Life after CPR—CNS damage, life support etc • Poor Quality of Life before CPR—It’s NOT good to be alive
Reasons to Refuse CPR • Patient is Dying—”Dying” causes cardiac arrest (not other way around) • Poor Quality of Life after CPR— Clinical determination (+ pt/surrogate) • Poor Quality of Life before CPR — Patient/surrogate assessment
NYS DNR Law (c) A surrogate may consent to an order not to resuscitate on behalf of an adult patient only if there has been a determination by an attending physician with the concurrence of another physician selected by a person authorized by the hospital to make such selection, given after personal examination of the patient that, to a reasonable degree of medical certainty:
NYS DNR Law • the patient has a terminal condition; or • the patient is permanently unconscious; or • resuscitation would be medically futile; or • resuscitation would impose an extraordinary burden on the patient in light of the patient's medical condition and the expected outcome of resuscitation for the patient.
Symbolic Nature of CPR • Icon of aggressive care—both good and bad • Full code = fighting back • DNR = giving up
Symbolic Nature of CPR • Patient/Family Attitude—doubtful that patient/family who wish full code really accept reality of fatal illness • Physician/Staff Attitude—presence of DNR order implies desire for less aggressive treatment in other realms
DNR and non-CPR Care • Physician/Staff Attitude—presence of DNR order implies desire for less aggressive treatment in other realms • Beach MC, Morrison SR, The Effect of Do-Not-Resuscitate Orders on Physician Decision-Making. J Am Geriatr Soc (2002) 50:2057–2061,.
DNR and non-CPR CareBeach and Morrison • Physician survey • 3 Clinical vignettes • 2 Versions of each • One with DNR • Other no DNR • Sequential treatment decisions
Reasons to Refuse CPR Cynical • Because the physician approaching the patient/family thinks it’s a good idea and persuades the decision maker • Gory details (“break your ribs”) • Often no mention of survival/outcome data
Rational Approach Choudhry NK, Choudhry S, Singer PA.CPR for Patients Labeled DNR: The Role of the Limited Aggressive Therapy Order. Ann Intern Med (2003) 138:65-68. • Presumes people make DNR decisions based on probability of poor outcome with CPR. • Overlooks high-yield circumstances (relatively good outcomes with CPR): • Witnessed “shockable” rhythms • CPR in OR • Iatrogenic/procedures
Rational Approach • Witnessed “shockable” rhythms • CPR in OR • Iatrogenic/procedures Choudhry: • LATO order: Limited aggressive therapy; • Intermediate status. • Unwieldy Short Code.
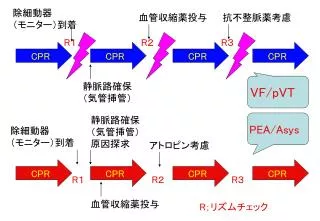
Code Duration and Outcome • Variety of outcome measures • Restoration of spontaneous circulation • Survival at 24 hours • Survival to discharge • Variety of timeframes • < or > 5, 10, 15, 20 min • Ranges (5-10, 11-15, 16-20 etc) • Mean CPR time among survival
Short Code • Allows patient to avoid outcomes of prolonged code • Eliminates generalizing DNR to other decisions • NOT a sham code ( “slow code,” “show code”) • NOT a partial code (“CPR but DNI”) • Go all out—but for less time • No confusion in initiating code • No confusion in running of code • No confusion in ending code