Download
1 / 12
120 likes | 288 Vues
ADDRESSING DEPARTMENTAL PAIN MEDICINE ISSUES 1997-2002. Raymond C. Roy, PhD, MD Professor & Chair of Anesthesiology Wake Forest University School of Medicine Bowman Gray Campus Winston-Salem, NC 27157 rroy@wfubmc.edu. CHRONIC Outpatient (PCC) Inpatient Consults ACUTE

E N D
ADDRESSING DEPARTMENTAL PAIN MEDICINE ISSUES 1997-2002 Raymond C. Roy, PhD, MD Professor & Chair of Anesthesiology Wake Forest University School of Medicine Bowman Gray Campus Winston-Salem, NC 27157 rroy@wfubmc.edu
CHRONIC Outpatient (PCC) Inpatient Consults ACUTE Acute Pain Service (APS) Number of FTE’s FacFelResEmpl* 4 3 1-2 26 + + + + 1 1 1-2 2 *includes clinical research FTE’s +divided between PCC & APS PAIN MEDICINE - 1997
PAIN MEDICINE ISSUES - 1998 • PCC losing $$$$ • Faculty accountability • Compliance • Inconsistent acute pain service (APS) • Uninspired APS • Disconnect between OR, PACU & APS
“OPPORTUNITIES” TO REVERSE PAIN $$$$ LOSSES • Renegotiate contracts • Billing & collecting • documentation, coding • Management & #employees • Faculty behavior • Patient mix • E&M vs procedure, study vs non-study, “good” vs “bad” insurance • Facility fees • MD- vs hospital-based
FACULTY BEHAVIOR • Unacceptable clinic cancellation rate • Conflict of interest • WFU salary/time vs consulting fees/time • Inaccurate accounting for time • clinical, academic, meeting, vacation • Documentation • compliance (Medicare audit risk)
STEPS TAKEN • Reduced # pain faculty on payroll 7 -> 2 • Established private practice relationship • New (excellent) clinic manager • Reduced # PCC employees 27 -> 8 • “Weeding out” inappropriate patients • Improved documentation, coding • Dept Chair – regular Friday am pain clinic • Negotiating to be “hospital-based” clinic
RELATIONSHIP WITH PRIVATE GROUP (Hospital-based) • Private group head– former PCC head • Non-salaried clinical appointments • Academic support • Malpractice - consults, vacation coverage • Joint conferences • 2 Fellows per month • Private group head – Co-I NIH Pain Center Grant
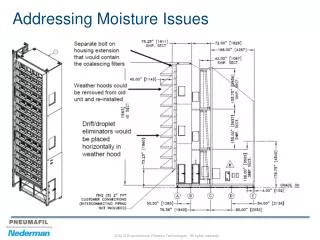
ADVANTAGES OF BEING “HOSPITAL-BASED” • Facility fee to cover overhead • Hospital provides ancillaries • Better equipment • More & better space
CHRONIC Outpatient (PCC) Inpatient Consults Private Clinic ACUTE Reg Anes Block Acute Pain Service (APS) Number of FTE’s FacFelResEmpl 1 2 1-2 7 + + + + 4 2 0 1 0 2 (1) 1 0 2 1 PAIN MEDICINE - 2001
SUMMARY • PCC losses decreased • Pain Fellowship • “Much better!” (fellows) • RRC visit in 2000– 5 yr approval • “Seamless” - regional anesthesia block, OR, PACU, and APS • Outstanding regional anesthesia block • Sustained relationship with private sector • Hospital-based clinic negotiations • Ready to recruit pain MD FTE in 2002