Download

1 / 32
320 likes | 601 Vues
Clubfoot deformation of the shape of the foot and impairment of function. Clubfoot Etiology. Unknown Most likely a combination of genetic and environmental factors. Incidence. 0,4- 1:1000 live births Male : Female 2:1 50% Bilatera l. Location of deformity.

E N D
Clubfoot deformation of the shape of the foot and impairment of function
ClubfootEtiology • Unknown • Most likely a combination of genetic and environmental factors
Incidence • 0,4-1:1000 live births • Male : Female 2:1 • 50% Bilateral
Location of deformity • Forefoot-phalanges and metatarsal • Midfoot-cuboid navicular cuneiforms • Hindfoot-talus calcaneus
Plane of deformity • In the hindfoot, coronalrotation produces heel varus (medial) or valgus (lateral) • Sagital plane rotation of the the hindfoot produced equinus (plantarflexion) or calcaneus (dorsiflexion)
Plane of deformity • Coronal rotation of the midfoot and forefoot is discribed as adduction or abduction as it relates to medial or laterl deviation of the foot
Plane of deformity • Pronation and supination are axial rotations through the midfoot and the midfoot-forefoot articulation
Pathology – bones Talus abnormal relationships including: • anterior extrusion of the body of the talus • external rotation of the body in the ankle mortise, equinus • medial and plantar deviation of the neck of the talus
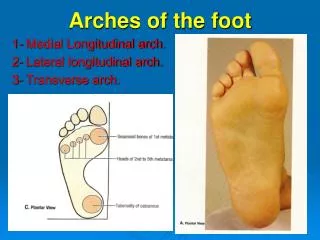
Pathology – bones • Calcaneus - Equinus, varus, medial rotation • Navicular, cuboid – medial subluxation • Forefoot - adducted and supinated, cavus in severe cases • Femur, tibia and fibula - the entire lower limb can be shorter
Pathology – muscles • Imbalance of type I and II, fibrosis caused by infiltration of fibroblast • Atrophy of the leg especially in peroneal group, triceps surae, tibialis posterior, FDL,FHL are contracted
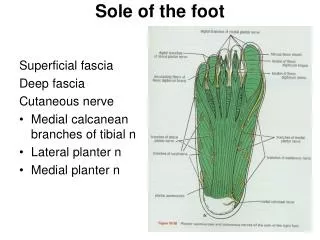
Pathology - soft tissues • Abnoraml colagen structure • Tendon sheaths - o frequently thickened • Joint capsules – severe cases: contractures of ankle, subtalar, talonavicular, calcaneocuboid • Ligaments - severe cases: contractures of calcaneofibular + talofibular ligs, deltoid lig, long and short plantar ligs, spring lig, long plantar lig. (bifurcate lig) • Fascia - contracture of fascial planes and of plantar fascia
Classification • Postural - postural or positional talipes can be passively fully corrected or even overcorrected • Fixed 1. Flexible 2. Resistant
Classification – Dimeglio • soft-soft – postural (20%) • soft-stiff – correction in saggital and horizontal planes over 50%, hindfoot varus 20 (33%) • stiff-soft - correction in saggital and horizontal planes below 50% (35%) • stiff-stiff – correction of equinus and varus less than 20%, hindfoot varus 45 (12%)
Treatment • Treatment and outcomes depends on degree of deformation • Non-operative • Operative
Non-operative • Series of redression casts applied as early as first 7-10 of life • Casts changed every 7-14 days • Post treatment options: lower leg splinters, Dennis-Brown orthosis, footwear, physiotherapy • Ponseti method – Achilles tenotomy • After 6-12 weeks x-ray control
Operative treatment • Time of surgery – 6-12 months • Type IV – no conservative treatment • Restoration of correct position of bones
Operative treatment • Posterior release • Posteromedial release • Posteromedial and lateral release • Complete peritalar release
Residual deformities • Forfoot adductus – opening wedge osteotomy of cuboid, closing wedge osteotomy of calcaneus, partial resection of calcaneus Lichtblau, calcaneo-cuboid arthrodesis Evans, • Foot cavus – osteotomy of cvalcaneus Dwyer and Dwyer II • Over 12 years – triple arthrodesis • Ilizarov method – secondary correction
Metatarsus adductus • MA is medial deviation of the forefoot at the level of the midtarsal joints • Etiology not completely understood-packing abnormalities (abnormal mechanical intrauterine forces)
Metatarsus adductustreatment • Spontaneus resolution-only observation • Home stretching program • Serial casts • Surgery
CONGENITAL FLATFOOT (Planovalgus) • Deformity consisting: • Hindfoot valgus • Midfoot supination and abduction • Deviation of plantar arch • Treatment- surgery
Calcaneovalgus foot • The foot is in extreme dorsiflexion • Treatment: • Home stretching program • Serial casts • Surgery