Download

1 / 38
500 likes | 2.24k Vues
Approach to the patient with headache. Zhang Lei 张磊 Dept. Neurology 1st hosp WenZhou Medical College. Classification. Acute headache — including all kinds of the onset of headache Chronic and recurrent headache — migraine, tension-type headache,

E N D
Approach to the patient with headache Zhang Lei 张磊 Dept. Neurology 1st hosp WenZhou Medical College
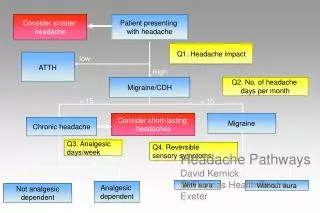
Classification • Acute headache — including all kinds of the onset of headache • Chronic and recurrent headache — migraine, tension-type headache, cluster headache and chronic daily headache
The primary goal of the evaluation • accurate distinction of benign headache syndromes from serious organic pathologies
Acute headache • Acute headache is the most common resons for visit to EM. • Primary headache: such as …… primary manifestation and no underlying disease process is present • Secondary headache: is a condition in which ……
Challenge to the clinician facing with acute headache • Performing expensive battery of tests? • To certain headache patients with life-threatening but treatable diseases , failure to performe tests means …… • Challenge to the clinician in EM or Dept. of Neurology is ……
The primary goals in managing patients with acute headache • Three same goals apply for patients with primary or secondary headache — diagnose the cause of headache —provide emergency therapy —provide the patient with a means of long-term care
Pathophysiology in primary headache • The precise mechanisms involved in the initiation of a migraine headache are not completely understood. • There appears to be general agreement that a key element is changes in the blood flow within the brain that become oversensitive to a variety of triggers.
Pathophysiology in primary headache • External stimulus = trigger e.g., certain foods (caffeine, chocolate, pepper, capsicum) alcohol or nitrites stress or stress letdown, emotinal factor lack of sleep or hunger hormonal fluctuation smoke, scents or fumes exercise
Pathophysiology in secondary headache • External stimulus = disease state e.g., increased ICP(intracranial pressure) cerebral hemorrhage vascular malformation meningitis giant-cell arteries nitrates and other vasoactive drugs low cerebrospinal fluid pressure
History of the headache • Previous history of headache — maybe the most important historical information to determine — a history of similar headache for many years suggest a primary — a second headache is much more likely as following :
Previous history of headache • If is the first headache in the life • if it is the worst headache • if is different in character from past headache • if it is persistent despite the use of measures that could relieved as before
Age of onset • primary headache —Age of onset childhood to younger adulthood • suspicious for secondary headache — onset at an age greater than 50 years e.g., hypertension.
Activity at onset of headache • occurs with lifting, straining, or squatting • headache during coitus, coital migraine • worse in the supine position • improve in supine position but worse on sitting and standing • worse or relieve in some special head position (cysticercosis)
Headache characteristics • Severity : “the worst headache in my life” SAH, TB meningitis • Temporal onset of pain: sudden onset or gradual onset • Location: location and radiation is nonspecific
Headache characteristics • Associated symptoms: Nausea, vomiting; —photophobia and phonophobia; — neck stiffness; changes in consciousness; — focal neurologic sign: aphasia, visual symptoms, ataxia, hemiparesis, etc —Fever, diaphoresis chill
Family history of headache • Is important but difficult to obtain in EM • pain and nausea and may have cognitive dysfountion • it is common that the patient not to be aware of family history ; or too young to realize • the patient can’t tell the migraine from “tension” or “sinus” hedache
Physical examination • Vital signs: Fever, Arterial hypertension (as the cause or the result) • General apperence: Cachexia, see in the patients with cancer, AIDS, TB, abscess • Head: e.g., poor denition, skull trauma, temporal tende -ness;
Physical examination • Neck: meningeal signs — nuchal rigidity ( neck stiffness in the anteroposterior direction ) — Kernig’s sign ( inability to extend the knee after passive hip flexion in the supine position) — Brudzinski’ sign (involuntary hip flexion after passive flexion of the neck in the supine position
Neurologic examination • Is normal in patient with primary headache • change in consciousness and focal dificit • funduscopic examination— papilledema (swollen disk) — high ICP
Laboratory studies • Blood evaluation: including complete blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), thyroid function tests, drug screen(cocaine, amphetamine) • computed tomography • magnetic resonance imaging • magnetic resonance angiography
Lumbar puncture ( LP ) • LP and CSF analysis Indications: acute or chronic meningitis, SAH, low-CSF-pressure headache • Timing in relation to CT • CSF Analysis
CSF analysis • Opening pressure : high or low • SAH suspected : obtain cell counts in the first and last tubes ; also test for xanthochroism (persist for up to 2 weeks ) • Cultures for bacteria , TB , or fungus . • Cancer, cytologic analysis need 10 cc CSF .
Differential diagnosis • SAH : is frequently missed (25%) be alert to the mild hedache ,if CT is normal, LP is mandatory. • Meningitis: be missed as flu • Intracerebral hemorrhage e.g., cerebellum, no hemiparalysis
Differential diagnosis • Deep cerebral venous thrombosis(DCVT) • dental abscess • Trigeminal neuralgia sharp or burning pain • Low-CSF-pressure headache • Arterial hypertension
Differential diagnosis • Cysticercosis is the most common parasitic infection of the human CNS • is endemic in Mexico, Central and South America, India, and China • Immigration to the United States has resulted in an increased prevalence of this disease in the United States
Cysticercosis • Intracranially, the oncospheres may burrow into brain parenchyma, meninges, ependyma, and choroid plexus. • There are four patterns of neurocysticercosis: parenchymal, subarachnoid, intraventricular, and mixed. The parenchymal type is probably the most common
MIGRAINE HEADACHE • vary from person to person • usually characterized by • accompanied by a multitude of other symptoms • include nausea and vomiting, light sensitivity and distorted vision, dizziness, fever and chills
MIGRAINE HEADACHE • two most prevalent types • classic and common migraine • The difference is aura • occur about 10 to 30 minutes before the onset • includes temporary changes in vision
MIGRAINE HEADACHE • The early warning signs —due to a narrowing of the blood vessels • pain experienced —due to the subsequent expanding or dilating • results in the release of pain-producing substances
Triggering factors for migraines • Hormonal changes (particularly associated with menstruation and oral contraceptive use) • Sudden changes in the weather conditions • Certain foods or food additives, especially preservatives, MSG, caffeine, chocolate, cheese and corn products
Triggering factors for migraines • Strong odors, glaring lights • Cigarette smoke • Emotional factors • Changes in sleep patterns
How are migraine headaches treated? • relieve symptoms and to prevent future headaches from occurring. • Simple analgesics: Aspirin and Tylenol • Nonsteroidal Anti -Inflammatory Drugs naproxen 萘普生 ibuprofen 布洛芬 indomethacin 消炎痛
How are migraine headaches treated? • Ergot Derivatives : a vasoconstrictor that helps counteract the painful dilation stage of a migraine headache
How are migraine headaches treated? • Sumatriptan: represents one of the newer classes of drugs • characterized as a selective 5-HT1-receptor agonist and has proven effective in controlling migraine symptoms.
How are migraine headaches treated? • Beta-Blockers • Calcium Channel Blockers • Tricyclic Antidepressants • Anticonvulsants • Narcotic analgesics.
How are migraine headaches treated? • Medications for the treatment of migraines are often combined with biofeedback and relaxation training( yogo and qigong) • Diet restrictions have proven helpful for some migraine sufferers