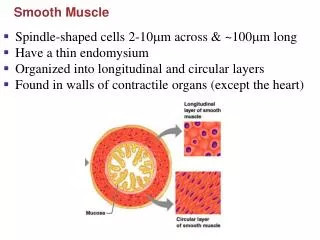
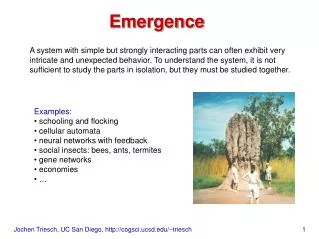
A Smooth emergence
A Smooth emergence. Jerod Schell, SRNA Oakland University-Beaumont Hospital Graduate Program of Nurse Anesthesia. Lidocaine vs. Alfentanil: its uses perioperatively. Why so concerned? What is the incidence of coughing on emergence from general anesthesia (GA) with an endotracheal tube??

A Smooth emergence
E N D
Presentation Transcript
A Smooth emergence Jerod Schell, SRNA Oakland University-Beaumont Hospital Graduate Program of Nurse Anesthesia Lidocaine vs. Alfentanil: its uses perioperatively
Why so concerned? What is the incidence of coughing on emergence from general anesthesia (GA) with an endotracheal tube?? Adverse side effects: HTN, tachycardia, tachyarrhythmia, ICP, IOP to name a few… Current methods for a smooth emergence = deep extubation, lidocaine jelly, LITA, short acting opioids.
Research Study Info: • Sadegi, M., Firozian, A., Ghafari, M.H. and Esfehani, F. (2008). • Comparison in Effect of Intravenous Alfentanil and Lidocaine on Airway-Circulatory Reflexes during Extubation. • International Journal of Pharmacology. 4(3). 223-226. • Dr. Ali Shariati Hospital, Medical Sciences/University of Tehran, Iran.
Materials with Inclusion/Exclusion: • RCT, double-blind study • Female patients undergoing Cesarean Section with ETT GA. • Ages 18-35 • ASA I or II ----------------------------------------------------------------- • Respiratory Disease, recent URI, previous laryngeal pathology or surgery, CAD, HTN (taking cardiac meds), smokers, opioid addiction, local anesthetic allergy – All Excluded.
Methods: • Standard Induction using Thiopental and Succinylcholine 1.5 mg/kg. • Used cuffed 7.0 mm OET, inflated with 2 ml greater than minimal leak pressure • GA with Isoflurane at 1 MAC before delivery and 0.5 MAC after, with Oxygen and Nitrous Oxide (50%). Muscle relaxant sustained with Atracurium then IV morphine given after birth. • After delivery, anesthetic gases turned off, oropharynx suctioned then 100% oxygen delivered for remainder of case. • Then……
Now the actual experiment… • “Randomly generated computer assignment” • 15 mcg/kg Alfentanil -or- • 1.5 mg/kg 2% Lidocaine IV Anesthetists would administer the given dose after return of spontaneous respiration, then after 2 minutes the patient was extubated.
What was measured? • Systolic and Diastolic BP • Heart Rate • Cough: yes or no. -Hemodynamics measured 2 minutes after the end of surgery and served as baseline values Then re-assessments 2 minutes after study drug given and 1 minute after extubation with comparisons made.
Hemodynamic Statistics Statistically significant data for both categories except baseline values.
Statistical analysis • Distribution was checked by Kolmogorov Test • Statistical comparison by T-test, Mann-Whitney U-test, and Chi-square Test. • Significant when P <.05, two tailed.
How were subjects treated?? • Narcotics and Lidocaine are both used in practice today, merely a comparison to current acceptable therapies. • Typically do not have scheduled Cesarean Sections with a GETA…
Study Notes: Discussion • No patients excluded • No laryngospasm or bronchospasm • Negative effects avoided: -Stress reactions -Intracranial, Intrabdominal pressure -Avoid bleeding or severe injury during emergence.
Study Notes (cont.) • Controlled timing very well. • Previous Lidocaine studies cannot statistically prove an improved emergence, only clinical experience with practitioners. • Narcotic delay?? -No clinically significant delay in emergence with narcotic use.
Study Limitations: • Narrow patient population • Healthy individuals • Not all institutions use Alfentanil
Can we use this tomorrow? • Alfentanil = opioid agonist -Precaution with Respiratory disease, can use as surgical anesthesia or analgesia. • Cost: 500 mcg/ml = $5.26 per ml. • - about $10 per 70 kg patient.
The Art of Anesthesia…. Emergence